LH Lab Test
-
How to Stop TRT with Post Cycle Therapy (PCT)
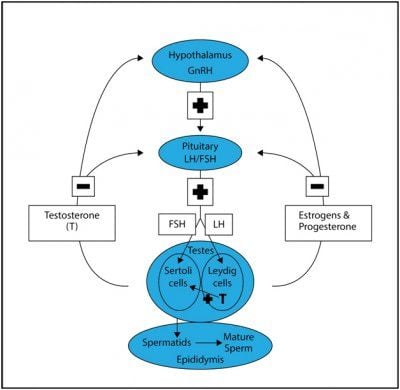
Categories: Testosterone Tests , Testosterone Side Effect Management , TRT Side Effects , Testosterone Blood Tests , Testosterone Lab Tests , LH Lab Test , FSH Fertility Test , Bodybuilder lab testsHow to Safely Use PCT After TRT: Stopping Testosterone Replacement Therapy Table of Contents What is Post Cycle Therapy PCT? Why Do Men Stop TRT? Common reasons a man may need to discontinue TRT include: Normalizing Natural Testosterone After Stopping TRT PCT Treatments to Jump Start Natural Testosterone and Sperm Production How to Know if Your PCT Worked? Buy Discounted Lab's Post-PCT Panel References: There is a common phrase most men will hear when they consider testosterone replacement therapy (TRT); it may be something they hear from friends or often what they read online: "TRT is for life." There is an element of truth to this statement: when a man has low testosterone, in order to treat it and maintain healthy or optimal levels, he will always need TRT to achieve it. However, saying "it's for life" remains a somewhat inaccurate statement, and this is where we enter into the realm of what is commonly referred to as Post Cycle Therapy or PCT. TRT and anabolic androgenic steroids (AAS) can lead to dysfunction in HPTA (Hypothalamic-Pituitary-Testicular Axis). Supplemental testosterone can inhibit the release of the body's own testosterone production through negative feedback inhibition on LH levels. This feedback inhibition also results in the suppression of FSH levels, leading to the suppression of sperm production (spermatogenesis). During recent years a large surge in testosterone prescriptions and TRT clinics has unfortunately led to many men who have been misdiagnosed with low testosterone yet placed on TRT when it may not have been needed in the first place. If you are one of these men and you are considering discontinuing testosterone treatments, some protocols can help restore your hormone axis. You do not want to stop testosterone "cold turkey," which will lead to unnecessary symptoms that could last for many months. Understanding TRT and Its Impact on the Body Testosterone Replacement Therapy (TRT) can be a game-changer for men with low testosterone levels, but it's crucial to understand how it impacts the body. TRT involves introducing exogenous testosterone into the body, which can disrupt the natural hormone production process. To grasp the full picture, we need to explore the Hypothalamic-Pituitary-Testicular Axis (HPTA) and how TRT affects it. The Hypothalamic-Pituitary-Testicular Axis and TRT The Hypothalamic-Pituitary-Testicular Axis (HPTA) is a sophisticated system that regulates testosterone production. It starts with the hypothalamus, which produces Gonadotropin-Releasing Hormone (GnRH). This hormone signals the pituitary gland to release Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH). LH and FSH then stimulate the testes to produce testosterone. When you undergo Testosterone Replacement Therapy (TRT), this delicate balance can be disrupted. The introduction of exogenous testosterone can suppress the body's natural production of LH and FSH, leading to a decrease in the body's ability to produce testosterone on its own. Impact of TRT on Natural Testosterone Production The impact of TRT on natural testosterone production can be significant. When exogenous testosterone is introduced, it can lead to a suppression of LH and FSH, which are crucial for natural testosterone production. This suppression can result in various symptoms, such as low libido, fatigue, and decreased muscle mass. Over time, prolonged use of TRT can lead to hypogonadism, a condition where the testes are unable to produce sufficient testosterone. This is why understanding the effects of TRT on natural hormone production is essential for anyone considering or currently undergoing TRT. What is Post Cycle Therapy PCT? PCT is a treatment plan after discontinuing anabolic androgenic steroids (AAS). It is a phrase most commonly associated with what we might call "recreational steroid users" (RSU), such as bodybuilders: people who do not need steroid hormones like testosterone for medical reasons but use them for muscular competition advantage. In such cases, the individual will supplement with AAS for a set period of time, known as a steroid cycle, and then discontinue use. As his use of AAS shut down his natural testosterone production, just as it does with TRT, he will often implement a PCT plan for natural production to restart. Such plans will include Selective Estrogen Receptor Modulators (SERMs) or other items, such as the peptide HCG. The goal for the RSU, as eluded to prior, is to regain his natural production of testosterone as quickly and efficiently as possible. There is no guarantee this will work. There is no guarantee he will reach his previous levels before AAS use, although perhaps levels that accurate enough. Then we have the TRT patient; such an individual had low testosterone levels before he began administering exogenous testosterone. The use of testosterone, just as it did with the RSU, will stop his natural production. This is a factor that bothers many men, but let us keep in mind a very significant one: you already had low levels, your body was not able to produce enough, to begin with, and was not going to be able to, or you wouldn't be on TRT. Nonetheless, there are reasons some men may find they need to discontinue use, and when that occurs, a PCT plan may be in order. Such a plan will not address his primary issue, low testosterone, but the goal here is to get at least some natural production back online. Why Do Men Stop Testosterone Replacement Therapy? Common reasons a man may need to discontinue TRT include: Need for Fertility TRT Cost TRT Side Effects or Health Issues Of the three potential reasons to stop TRT, fertility is the overwhelming reason for most men. Along with suppressing natural testosterone production, TRT can also have a negative impact on sperm production. There was a time in history not that long ago when it was thought exogenous testosterone would be touted as a male contraceptive. This idea died out when many men using testosterone found they were still able to impregnate a female. While many men on testosterone were found to be severely lacking in this department, it wasn't enough or significant enough to market the hormone as an actual contraceptive. The other common reasons for discontinuing TRT are cost and side effects. These are the least common reasons in comparison to fertility needs or desires, but both are still possible. We all go through points in life where money can get a little tight; loss of a job, unexpected expenses – whatever the reason, if you find you need to stop, considering a PCT plan with your physician will make the transition easier. You're still going to have low testosterone levels in the end – remember, you already had them, or you wouldn't have started TRT in the first place – but you'll hopefully be in a better position than you would be without, and in time, when your situation improves, you'll be able to jump back on your TRT plan. The same may hold true for the individual who has side effect issues. This will be the least common reason for discontinuation of TRT but certainly within the realm of possibility. You could be one of the rare individuals who cannot control his hematocrit even with regular therapeutic phlebotomy. You could be someone that has other health concerns and, for whatever reason, need to discontinue use until you figure out what's going on with your body. Hormonal imbalances, such as elevated estrogen levels, can also occur when stopping TRT, leading to conditions like gynecomastia. As was with the individual who was experiencing income issues, a PCT plan may be in order. Preparing for TRT Discontinuation Deciding to discontinue TRT is a significant step and should be approached with caution. One of the most critical aspects of stopping TRT safely is to do so under the guidance of a medical professional. Abruptly stopping TRT can lead to severe withdrawal symptoms and a dramatic drop in testosterone levels, which can be detrimental to your health. Gradual Tapering Under Medical Supervision When it comes to discontinuing TRT, gradual tapering is the safest approach. This process involves slowly reducing the dosage and frequency of testosterone administration to allow the body to adjust and begin producing testosterone naturally again. A healthcare provider can create a personalized tapering schedule based on factors such as the dosage and duration of your TRT use. This might involve reducing the amount of testosterone you inject or apply through gels over a set period. Regular check-ups with your healthcare provider are crucial during this time to monitor your progress and make any necessary adjustments to your tapering plan. This careful and monitored approach helps minimize withdrawal symptoms and supports the body's natural transition back to producing testosterone on its own. By understanding the impact of TRT on your body and following a medically supervised tapering plan, you can safely discontinue TRT and support your body's return to natural testosterone production. Normalizing Natural Testosterone After Stopping TRT For most men, studies have shown that for men who stop TRT, natural testosterone production can normalize within three months or longer, and spermiogenesis in well over a year. This is certainly not optimal when conception is the goal, which leads to the possible need for a PCT protocol. Post cycle therapy (PCT) is crucial in maintaining and recovering natural testosterone levels after using performance-enhancing drugs, as it helps enhance the body's own testosterone production. PCT Treatments to Restore Hormonal Balance and Jump Start Natural Testosterone and Sperm Production The use of the SERMs has been shown to increase testosterone levels to baseline in as little as 2-4 weeks. Studies have also shown spermiogenesis to improve significantly within 3-6 months. Clomid as we can easily see, greatly improves the time frames of recovery of these two important factors related to conceiving (testosterone and semen). PCT is crucial to restore hormonal balance, helping individuals recover from the use of anabolic steroids by promoting natural testosterone production and mitigating adverse effects caused by hormonal imbalances. HCG is another item commonly used in PCT for fertility purposes. HCG PCT has the ability to stimulate both testosterone production and spermiogenesis. It is not uncommon for fertility specialists to try both Clomid and HCG and, in some cases, in conjunction with one another. Unfortunately, there is much controversy among many fertility specialists regarding how much HCG should be administered for this purpose. While many physicians will prescribe SERMs in the range of 25-50mg per day to every other day, commonly prescribed HCG doses can run anywhere from 1000iu per day to 2500iu or even larger doses split into every other day schedules. Other common drugs used in this treatment, but to a lesser extent, include the SERM Tamoxifen Citrate, best known by its most notable trade name, Nolvadex. Treatments usually requires 4 weeks. Unfortunately, for some men, a PCT plan that includes some or all of these medications will not work. A HCG PCT plan is most likely to work in a TRT patient who is receiving treatment due to secondary hypogonadism. If a PCT plan has not worked – testosterone levels and sperm count have not increased – it is likely that the individual has primary hypogonadism, and as a result, will be best served (quality of life) by remaining on TRT. It's imperative to note: this individual had primary hypogonadism prior to beginning TRT, he did not obtain it because of TRT. How to Know if Your PCT Worked? After going through PCT, physicians tend to check your testosterone blood levels and upstream hormones like LH and FSH to determine if your hormone axis has been restored. Discounted Labs has created a Post PCT Lab Test Panel that makes it easy for men to know if their PCT has successfully worked. This lab test panel is designed to measure the health and recovery of the Hypothalamic-Pituitary-Testicular Axis (HPTA) after attempting to normalize it spontaneously or with the use of Post Cycle Therapy (PCT) (with the use of clomiphene, hCG, and other treatments) It is suggested that this panel be done no sooner than 4 weeks after PCT cessation and in a fasting state. You should fast for 12 hours before collection of the specimen. Fasting is defined as no consumption of food or beverage other than water for at least 12 hours before testing. If using a testosterone cream please be sure you have not rubbed any into the antecubital area of your arm for the last 24 hours as it can give elevated results. Lab tests included in the post-PCTest Panel: Ultra Sensitive Estradiol Test by Liquid Chromatography/Mass Spectrometry (LC/MS assay used to measure estradiol in men more accurately estradiol in men) Total and Free Testosterone LC/MS- No upper limit Luteinizing Hormone (LH) (responsible for activating Leydig testicular cells to produce your own testosterone). This hormone is shut down by testosterone replacement or AAS. Follicle Stimulating Hormone (FSH) (Responsible for activating Sertoli testicular cells to produce sperm). This hormone is shut down by testosterone replacement or AAS. CBC - Complete Blood Count (Includes hematocrit- red blood cell volume) CMP - Comprehensive Metabolic Panel (Includes liver and kidney function, glucose and electrolytes) For any man, simply discontinuing the use of testosterone can be difficult, to put it mildly. Your testosterone levels will completely bottom out when going the cold-turkey route, and this often. This severe sexual dysfunction, decreased energy, and even depression, to name a few of the consequences. Your levels may go up enough to at least function, to a degree, but it's going to take an enormous amount of time, as previously discussed. Cutting this time down significantly, and giving your body a boost in testosterone during the therapy process, is the only means of discontinuation that makes any sense, meaning some form of a PCT plan is a sensible approach. Buy Discounted Lab's Post-PCT Panel References: Diagnosis and Management of Anabolic Androgenic Steroid Use Testosterone Use in the Male Infertility Population: Prescribing Patterns and Effects on Semen and Hormonal Parameters How to Stop TRT Safely -
Key Pituitary And Thyroid Hormone Tests Before Starting Testosterone
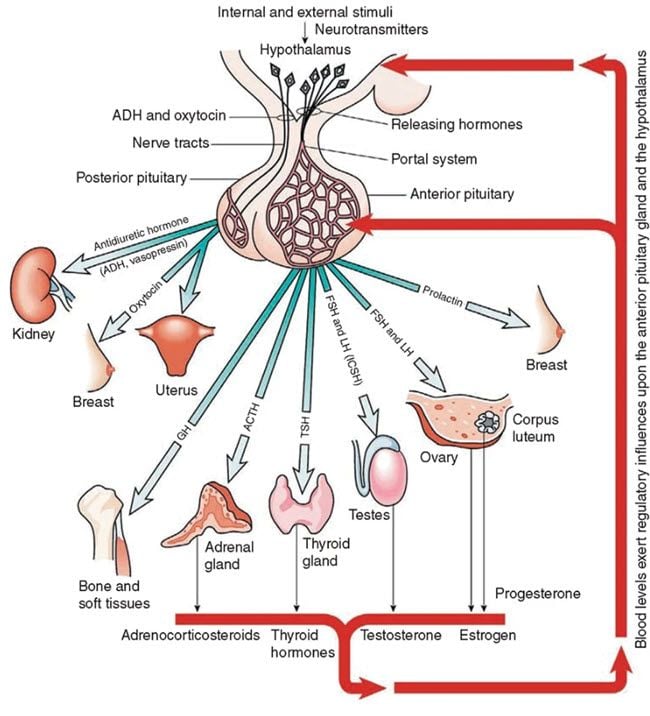
Categories: Testosterone Tests , Thyroid Lab Tests , TSH Thyroid Test , Free T3 Thyroid Test , Free T4 Thyroid Test , Reverse T3 Thyroid Test , Testosterone Side Effect Management , TRT Side Effects , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , TRT Testing , TRT Monitoring , Testosterone Replacement Monitoring Tests , Thyroid Tests , LH Lab Test , FSH Fertility Test , Prolactin Lab TestTable of Contents Symptoms Of Hypogonadism (Low Testosterone) And How To Diagnose Primary and secondary hypogonadism (Low Testosterone) The pituitary gland and problems associated with it Exploring Hyperprolactinemia (High Prolactin) and Its Implications in Low Testosterone Throwing a spotlight on the pituitary and its function Pituitary imaging in the diagnosis of low testosterone Learning about thyroid and its role in low testosterone Conclusions Testosterone replacement therapy is available in many forms and can be beneficial for men who have low testosterone levels. When the body doesn't produce enough testosterone (a condition also known as hypogonadism), men can experience different symptoms such as low sex drive, fatigue, bad mood, and irritability. The body might not produce enough testosterone because of different factors. For example, the pituitary and thyroid glands play an important role in the production of testosterone and if they are not healthy, young men might experience low testosterone levels. It is important to note here that the production of testosterone decreases as men age and this is normal to be so. However, approximately 0.1% of men aged 40-49 years and about 3-5% of men aged 60-79 develop androgen deficiency which can negatively influence their lifestyle. Those who have type 2 diabetes and are obese are at a higher risk of having low blood testosterone. Before taking advantage of testosterone replacement therapy, it is important to assess the health of other organs in the body which are directly related to the production of testosterone such as the pituitary and thyroid. The pituitary gland is a very small organ situated at the base of the skull, weighing just 0.018 oz. It is responsible for releasing the growth hormone as well with the production of testosterone. If a patient is suspected of having low testosterone levels, doctors usually recommend analyzing and treating the pituitary gland as well, before opting for testosterone replacement (TRT) therapy. Similarly, the thyroid is an endocrine gland situated in the neck. It is responsible for the production of numerous hormones which help the body's metabolic processes. It also plays a vital role in the production of testosterone. Symptoms Of Hypogonadism (Low Testosterone) And How To Diagnose This type of medical condition can have various symptoms and as mentioned earlier, people who are obese or have type 2 diabetes are more likely to develop hypogonadism. Other risk factors include chronic depression, cancer, a medicine which interferes with testosterone production, chronic illness, and others. People who abuse opiates and glucocorticoids are also at a higher risk of developing hypogonadism over time. Proper testosterone production is strictly correlated with a healthy lifestyle, which involves working out regularly and eating a balanced diet. Smoking and cardiovascular diseases can also put someone at risk of developing low blood testosterone. By improving the testosterone level through replacement therapy or by treating any existing pituitary or thyroid issue, the overall quality of life can be drastically increased. For example, men who have tried testosterone replacement therapy report better sexual satisfaction, better mood, more energy and a general sense of wellbeing. In very rare cases, the testosterone level can be low because of other factors, such as extremely hard physical training. Professional athletes, especially those who compete in combat sports, might have low testosterone levels as a result of fatigue, improper nutrition, lack of rest, etc. it is important to take a look at a patient's physical condition and training regime to accurately diagnose androgen deficiency. A professional can use special tests to diagnose hypogonadism. It is important to let an experienced healthcare provider assess the testosterone levels to avoid confusion and medical complications. Proper laboratory diagnosis is done early in the morning when testosterone levels are at their peak. For accurate screening, The Endocrine Society recommends two morning (8:00-10:00 a.m.) specimens obtained on different days. Testosterone production follows something called a diurnal rhythm, meaning that the production is higher in the morning and lower at the end of the day. Working night shifts or having poor quality sleep can drastically influence the result of the analysis, so patients should take this into consideration. Similarly, having an acute illness can also render false testosterone diagnosis. It is necessary to perform 2 or more testosterone evaluations to determine if a patient is suffering from hypogonadism or not, since approximately 33% of men have a positive result after one measurement. Evaluating testosterone levels is highly recommended for certain patients, regardless if they experience the hypogonadism symptoms or not. For example, patients with HIV or those who have type 2 diabetes mellitus, osteoporosis or chronic pulmonary disease are also at a higher risk of having low serum testosterone. Once the testosterone levels have been measured and it has been confirmed that the patient might benefit from testosterone replacement therapy, additional endocrinology tests should be performed to determine the nature of the hypogonadism – primary or secondary. Treating hypogonadism accurately is paramount, especially if the patient has certain fertility goals. Primary and secondary hypogonadism (Low Testosterone) As mentioned earlier, a low testosterone level in the bloodstream might result from 2 factors. The Leydig cells located in the testes are responsible for producing the majority of testosterone in men. This process takes place using the luteinizing hormone (LH) from the pituitary gland. The LH is also strictly linked to the GnRH which is produced by the hypothalamus. The GnRH is released in a pulsatile manner and a disruption in this process can lead to low testosterone levels over time. To sum it up, men can suffer from primary hypogonadism (the testosterone is not produced in the testes), from secondary hypogonadism (the production of LH or GnRH is disrupted in the pituitary or hypothalamus) or both. If a patient has primary hypogonadism, the LH and FSH levels will be elevated as these hormones are produced by the pituitary and hypothalamus but not properly converted into testosterone. Most specialists recommend karyotype analysis for further investigation. The causes of primary hypogonadism can be multiple and they include HIV, toxins gathered in the body, acquired anorchia, orchitis, and more. On the other hand, if the LH and FSH levels are low, then additional investigations must be done to determine the nature of the secondary hypogonadism. It basically means that the testes are perfectly capable of making testosterone, but they don't have the primary resource (LH) to do so. The pituitary gland and problems associated with it Secondary hypogonadism is a more complicated medical issue and it involves looking at the characteristics of the pituitary gland. There are numerous factors which might cause secondary hypogonadism such as certain types of tumors, untreated sleep apnea, infiltrative diseases, use of certain drugs such as marijuana, opiates, and heroin, etc. Hyperprolactinemia can be a contributing factor in about 5% of secondary hypogonadism. This means that a prolactin adenoma can put pressure on the pituitary gland and cause damage. There are also different types of medications which can affect prolactin secretion, such as metoclopramide and others. In some cases, secondary hypogonadism can be caused by GnRH deficiency which happens as a result of damage to the hypothalamus. This part of the brain can become injured as a result of toxins accumulation, trauma, taking certain types of medication, as well as systemic disease. If a patient is suspected of having secondary hypogonadism, he will receive a full pituitary workup to determine prolactin levels (which requires overnight fasting for 8-10 hours) and to see if its secretion is disrupted or not. It is paramount to differentiate between secondary hypogonadism originating in the pituitary and the one originating in the hypothalamus. Men who have fertility goals and want to have children in the near future need a different type of treatment than those who don't have any fertility goals. There are rare instances when men suffer from a combination of primary and secondary hypogonadism. This might happen as a result of alcohol abuse, sickle cell disease, and more. There are several treatment options available in this case such as spermatogenesis and others. Exploring Hyperprolactinemia (High Prolactin) and Its Implications in Low Testosterone It has been discovered that men who suffer from hyperprolactinemia experience a wide variety of symptoms, such as decreased sperm mobility and low libido. These can lead to a low-quality sex life and fertility problems. Even in the presence of relatively normal testosterone levels, hyperprolactinemia can have a significant negative impact on sexual health, leading to erectile dysfunction in worst cases. By normalizing prolactin levels, scientists have discovered that testosterone levels improve and the overall quality of life is enhanced as well. Correct prolactin levels are directly associated with a healthy testosterone metabolism. Therefore, patients who have low serum testosterone should seek treatment for improving prolactin levels first before opting for testosterone replacement therapy. Once it has been discovered that the body responds well to hyperprolactinemia treatment, it might not be necessary to take advantage of testosterone replacement therapy. Throwing a spotlight on the pituitary and its function The pituitary gland plays a vital role in the production of testosterone and it should be properly assessed to determine if there are any additional hormonal imbalances present in the body. For example, for men with a testosterone level lower than 150 ng/dL, an evaluation of the anterior pituitary axes is highly recommended. This evaluation can discover other medical conditions, such as hypopituitarism, which might affect proper testosterone production. Testing the pituitary gland should be done early in the morning before 9 am with overnight fasting (8-10 hours). This is done by drawing blood to measure cortisol levels as well as ACTH. If the patient works night shifts, which might compromise the accuracy of the test, an ACTH stimulant is administered intramuscularly. This test can give insights into the hormonal balance of the patient. For example, if it is suspected that the patient has Cushing syndrome, the doctor might recommend a 1 mg dexamethasone suppression test. If acromegaly is suspected (growth hormone deficiency), then other tests are necessary to determine the exact levels of growth hormone. Such tests are required to determine the full biochemical makeup of the patient in relation to the pituitary gland and hypogonadism. If the results are positive for one or more of those tests, the patient will be redirected to endocrinology for additional measurements. Pituitary imaging in the diagnosis of low testosterone Magnetic resonance imaging (MRI) might be used to discover further details about the pituitary gland and this decision is based on multiple tests of the hormone levels. Pituitary imaging is done only when proper clinical management is required and it can be used to discover incidentalomas, which can be 6 mm in diameter or less. These are small bodies that might grow on the pituitary gland and put pressure on it which in turn disrupts the regular flow of hormones required for healthy testosterone production. These incidentalomas are usually found in approximately 20% of autopsies and can also be encountered in up to 10% of the population who is referred to pituitary imaging. The MRI testing of the pituitary should be done on men who have severe secondary hypogonadism (testosterone levels are below 150 ng/dL, persistent hyperprolactinemia, and others). Pituitary imaging isn't necessary for cases of primary hypogonadism and it is only performed when absolutely necessary. Learning about thyroid and its role in low testosterone The thyroid is very important when it comes to testosterone production. In general terms, hypothyroidism has been associated with a decrease in total testosterone levels, while hyperthyroidism might lead to converting too much testosterone into estradiol, which results in impaired sexual function, gynecomastia (enlarged man's breasts), and other medical conditions. In some cases, hypothyroidism can lead to hyperprolactinemia, but such occurrences are rare. When this happens, improving the thyroid function through certain treatments or medication can stabilize prolactin levels and this, in turn, will normalize testosterone production. Hypothyroidism is also frequently associated with erectile dysfunction. Similarly, hyperthyroidism can also be problematic, as it has been associated with ejaculatory dysfunction, as shown in a study done on over 750 men. More than 50 percent of those who had hyperthyroidism also showed symptoms of reduced sperm mobility and ejaculatory problems. However, when these men received treatment for hyperthyroidism, their fertility and testosterone production improved significantly, which means that testosterone replacement therapy isn't necessarily the go-to treatment for all men suffering from androgen deficiency. Conclusions As presented in this article, the human body is very complex, and there might be multiple causes for a low serum testosterone level in the bloodstream on males of all ages. It is important to determine whether the hypogonadism is primary or secondary, as well as perform numerous tests and hormone evaluations to determine the nature of the hypogonadism and to prescribe the correct treatment. In case the pituitary gland is the culprit, MRI tests might be required, though such instances are rare. Certain types of treatments are also recommended if the patient has fertility goals. If none of the other medications and treatments for hypogonadism are accurate, then testosterone replacement therapy might be considered for certain patients. By the way, monitoring serum testosterone, LH, FSH and prolactin is very easy these days thanks to tests that can be bought online at discounted prices. Visit www.discountedlabs.com for more details.