How to Safely Use PCT After TRT: Stopping Testosterone Replacement Therapy
Table of Contents
There is a common phrase most men will hear when they consider testosterone replacement therapy (TRT); it may be something they hear from friends or often what they read online: "TRT is for life." There is an element of truth to this statement: when a man has low testosterone, in order to treat it and maintain healthy or optimal levels, he will always need TRT to achieve it. However, saying "it's for life" remains a somewhat inaccurate statement, and this is where we enter into the realm of what is commonly referred to as Post Cycle Therapy or PCT.
TRT and anabolic androgenic steroids (AAS) can lead to dysfunction in HPTA (Hypothalamic-Pituitary-Testicular Axis). Supplemental testosterone can inhibit the release of the body's own testosterone production through negative feedback inhibition on LH levels. This feedback inhibition also results in the suppression of FSH levels, leading to the suppression of sperm production (spermatogenesis).
During recent years a large surge in testosterone prescriptions and TRT clinics has unfortunately led to many men who have been misdiagnosed with low testosterone yet placed on TRT when it may not have been needed in the first place. If you are one of these men and you are considering discontinuing testosterone treatments, some protocols can help restore your hormone axis. You do not want to stop testosterone "cold turkey," which will lead to unnecessary symptoms that could last for many months.
Understanding TRT and Its Impact on the Body
Testosterone Replacement Therapy (TRT) can be a game-changer for men with low testosterone levels, but it's crucial to understand how it impacts the body. TRT involves introducing exogenous testosterone into the body, which can disrupt the natural hormone production process. To grasp the full picture, we need to explore the Hypothalamic-Pituitary-Testicular Axis (HPTA) and how TRT affects it.
The Hypothalamic-Pituitary-Testicular Axis and TRT
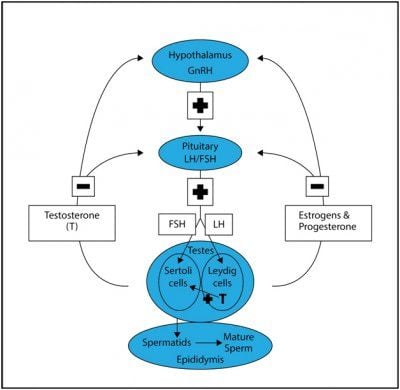
The Hypothalamic-Pituitary-Testicular Axis (HPTA) is a sophisticated system that regulates testosterone production. It starts with the hypothalamus, which produces Gonadotropin-Releasing Hormone (GnRH). This hormone signals the pituitary gland to release Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH). LH and FSH then stimulate the testes to produce testosterone. When you undergo Testosterone Replacement Therapy (TRT), this delicate balance can be disrupted. The introduction of exogenous testosterone can suppress the body's natural production of LH and FSH, leading to a decrease in the body's ability to produce testosterone on its own.
Impact of TRT on Natural Testosterone Production
The impact of TRT on natural testosterone production can be significant. When exogenous testosterone is introduced, it can lead to a suppression of LH and FSH, which are crucial for natural testosterone production. This suppression can result in various symptoms, such as low libido, fatigue, and decreased muscle mass. Over time, prolonged use of TRT can lead to hypogonadism, a condition where the testes are unable to produce sufficient testosterone. This is why understanding the effects of TRT on natural hormone production is essential for anyone considering or currently undergoing TRT.
What is Post Cycle Therapy PCT?
PCT is a treatment plan after discontinuing anabolic androgenic steroids (AAS). It is a phrase most commonly associated with what we might call "recreational steroid users" (RSU), such as bodybuilders: people who do not need steroid hormones like testosterone for medical reasons but use them for muscular competition advantage. In such cases, the individual will supplement with AAS for a set period of time, known as a steroid cycle, and then discontinue use. As his use of AAS shut down his natural testosterone production, just as it does with TRT, he will often implement a PCT plan for natural production to restart. Such plans will include Selective Estrogen Receptor Modulators (SERMs) or other items, such as the peptide HCG.
The goal for the RSU, as eluded to prior, is to regain his natural production of testosterone as quickly and efficiently as possible. There is no guarantee this will work. There is no guarantee he will reach his previous levels before AAS use, although perhaps levels that accurate enough.
Then we have the TRT patient; such an individual had low testosterone levels before he began administering exogenous testosterone. The use of testosterone, just as it did with the RSU, will stop his natural production. This is a factor that bothers many men, but let us keep in mind a very significant one: you already had low levels, your body was not able to produce enough, to begin with, and was not going to be able to, or you wouldn't be on TRT. Nonetheless, there are reasons some men may find they need to discontinue use, and when that occurs, a PCT plan may be in order. Such a plan will not address his primary issue, low testosterone, but the goal here is to get at least some natural production back online.
Why Do Men Stop Testosterone Replacement Therapy?
Common reasons a man may need to discontinue TRT include:
-
Need for Fertility
-
TRT Cost
-
TRT Side Effects or Health Issues
Of the three potential reasons to stop TRT, fertility is the overwhelming reason for most men. Along with suppressing natural testosterone production, TRT can also have a negative impact on sperm production. There was a time in history not that long ago when it was thought exogenous testosterone would be touted as a male contraceptive. This idea died out when many men using testosterone found they were still able to impregnate a female. While many men on testosterone were found to be severely lacking in this department, it wasn't enough or significant enough to market the hormone as an actual contraceptive.
The other common reasons for discontinuing TRT are cost and side effects. These are the least common reasons in comparison to fertility needs or desires, but both are still possible. We all go through points in life where money can get a little tight; loss of a job, unexpected expenses – whatever the reason, if you find you need to stop, considering a PCT plan with your physician will make the transition easier. You're still going to have low testosterone levels in the end – remember, you already had them, or you wouldn't have started TRT in the first place – but you'll hopefully be in a better position than you would be without, and in time, when your situation improves, you'll be able to jump back on your TRT plan.
The same may hold true for the individual who has side effect issues. This will be the least common reason for discontinuation of TRT but certainly within the realm of possibility. You could be one of the rare individuals who cannot control his hematocrit even with regular therapeutic phlebotomy. You could be someone that has other health concerns and, for whatever reason, need to discontinue use until you figure out what's going on with your body. Hormonal imbalances, such as elevated estrogen levels, can also occur when stopping TRT, leading to conditions like gynecomastia. As was with the individual who was experiencing income issues, a PCT plan may be in order.
Preparing for TRT Discontinuation
Deciding to discontinue TRT is a significant step and should be approached with caution. One of the most critical aspects of stopping TRT safely is to do so under the guidance of a medical professional. Abruptly stopping TRT can lead to severe withdrawal symptoms and a dramatic drop in testosterone levels, which can be detrimental to your health.
Gradual Tapering Under Medical Supervision
When it comes to discontinuing TRT, gradual tapering is the safest approach. This process involves slowly reducing the dosage and frequency of testosterone administration to allow the body to adjust and begin producing testosterone naturally again. A healthcare provider can create a personalized tapering schedule based on factors such as the dosage and duration of your TRT use. This might involve reducing the amount of testosterone you inject or apply through gels over a set period. Regular check-ups with your healthcare provider are crucial during this time to monitor your progress and make any necessary adjustments to your tapering plan. This careful and monitored approach helps minimize withdrawal symptoms and supports the body's natural transition back to producing testosterone on its own.
By understanding the impact of TRT on your body and following a medically supervised tapering plan, you can safely discontinue TRT and support your body's return to natural testosterone production.
Normalizing Natural Testosterone After Stopping TRT
For most men, studies have shown that for men who stop TRT, natural testosterone production can normalize within three months or longer, and spermiogenesis in well over a year. This is certainly not optimal when conception is the goal, which leads to the possible need for a PCT protocol. Post cycle therapy (PCT) is crucial in maintaining and recovering natural testosterone levels after using performance-enhancing drugs, as it helps enhance the body's own testosterone production.
PCT Treatments to Restore Hormonal Balance and Jump Start Natural Testosterone and Sperm Production
The use of the SERMs has been shown to increase testosterone levels to baseline in as little as 2-4 weeks. Studies have also shown spermiogenesis to improve significantly within 3-6 months. Clomid as we can easily see, greatly improves the time frames of recovery of these two important factors related to conceiving (testosterone and semen). PCT is crucial to restore hormonal balance, helping individuals recover from the use of anabolic steroids by promoting natural testosterone production and mitigating adverse effects caused by hormonal imbalances.
HCG is another item commonly used in PCT for fertility purposes. HCG PCT has the ability to stimulate both testosterone production and spermiogenesis. It is not uncommon for fertility specialists to try both Clomid and HCG and, in some cases, in conjunction with one another. Unfortunately, there is much controversy among many fertility specialists regarding how much HCG should be administered for this purpose. While many physicians will prescribe SERMs in the range of 25-50mg per day to every other day, commonly prescribed HCG doses can run anywhere from 1000iu per day to 2500iu or even larger doses split into every other day schedules. Other common drugs used in this treatment, but to a lesser extent, include the SERM Tamoxifen Citrate, best known by its most notable trade name, Nolvadex. Treatments usually requires 4 weeks.
Unfortunately, for some men, a PCT plan that includes some or all of these medications will not work. A HCG PCT plan is most likely to work in a TRT patient who is receiving treatment due to secondary hypogonadism. If a PCT plan has not worked – testosterone levels and sperm count have not increased – it is likely that the individual has primary hypogonadism, and as a result, will be best served (quality of life) by remaining on TRT. It's imperative to note: this individual had primary hypogonadism prior to beginning TRT, he did not obtain it because of TRT.
How to Know if Your PCT Worked?
After going through PCT, physicians tend to check your testosterone blood levels and upstream hormones like LH and FSH to determine if your hormone axis has been restored. Discounted Labs has created a Post PCT Lab Test Panel that makes it easy for men to know if their PCT has successfully worked.
This lab test panel is designed to measure the health and recovery of the Hypothalamic-Pituitary-Testicular Axis (HPTA) after attempting to normalize it spontaneously or with the use of Post Cycle Therapy (PCT) (with the use of clomiphene, hCG, and other treatments)
It is suggested that this panel be done no sooner than 4 weeks after PCT cessation and in a fasting state. You should fast for 12 hours before collection of the specimen. Fasting is defined as no consumption of food or beverage other than water for at least 12 hours before testing. If using a testosterone cream please be sure you have not rubbed any into the antecubital area of your arm for the last 24 hours as it can give elevated results.
Lab tests included in the post-PCTest Panel:
-
Ultra Sensitive Estradiol Test by Liquid Chromatography/Mass Spectrometry (LC/MS assay used to measure estradiol in men more accurately estradiol in men)
-
Total and Free Testosterone LC/MS- No upper limit
-
Luteinizing Hormone (LH) (responsible for activating Leydig testicular cells to produce your own testosterone). This hormone is shut down by testosterone replacement or AAS.
-
Follicle Stimulating Hormone (FSH) (Responsible for activating Sertoli testicular cells to produce sperm). This hormone is shut down by testosterone replacement or AAS.
-
CBC - Complete Blood Count (Includes hematocrit- red blood cell volume)
-
CMP - Comprehensive Metabolic Panel (Includes liver and kidney function, glucose and electrolytes)
For any man, simply discontinuing the use of testosterone can be difficult, to put it mildly. Your testosterone levels will completely bottom out when going the cold-turkey route, and this often. This severe sexual dysfunction, decreased energy, and even depression, to name a few of the consequences. Your levels may go up enough to at least function, to a degree, but it's going to take an enormous amount of time, as previously discussed. Cutting this time down significantly, and giving your body a boost in testosterone during the therapy process, is the only means of discontinuation that makes any sense, meaning some form of a PCT plan is a sensible approach.