Page 2 - Testosterone Tests
-
How to Lower High Hematocrit - Effective Strategies
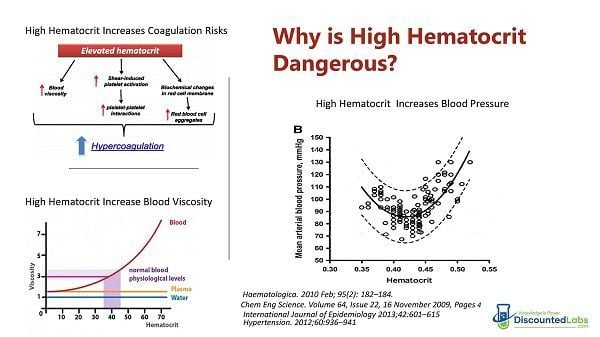
Categories: High Hematocrit , CBC Lab Panel , Testosterone Tests , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , Testosterone Replacement Monitoring TestsHigh hematocrit levels, which measure the percentage of red blood cells in the blood, can be signs of several underlying health conditions and they are also a common side effect of testosterone replacement therapy (TRT). High hematocrit levels can increase the risk of developing blood clots, strokes, and other serious complications, especially for those with an underlying condition. Low red blood cell levels, also known as low hematocrit levels, can indicate conditions such as anemia, while high red blood cell levels often signal dehydration and could indicate other conditions, such as polycythemia, increasing a person’s chance of developing blood clots or experiencing blood loss. We will review the different ways to lower the hematocrit and the number of red blood cells on TRT. How to Lower the High Hematocrit Caused by Testosterone Replacement Therapy (TRT) Testosterone replacement therapy (TRT) is one of the most effective ways to combat low testosterone levels, but it's vital that you understand the risks associated with the treatment. As with any form of hormone replacement therapy, there are a few downsides to receiving regular injections of testosterone. One of the main TRT side effects is increased hematocrit, also known as erythrocytosis, which can be a sign of androgen deficiency. This article will explain why this happens, the potential long-term health consequences, and how to prevent or manage this issue. Since abnormally high hematocrit values can pose serious health problems, this article will analyze the correlation between testosterone therapy and high hematocrit. TRT, sleep apnea, smoking, and red blood cell production are contributing factors that can cause high hematocrit that can increase cardiovascular risks if not properly managed. This article explains the basics of how to manage high hematocrit while using testosterone therapy. What is hematocrit? There are several standard ways to measure red blood cells: hematocrit, hemoglobin, and RBC (red blood cell count). All of these are related, and doctors will usually look at two or more. Hematocrit, also referred to as the proportion of red blood cells, is a measurement of how much of a person's blood is made up of red blood cells, also known as whole blood. Hemoglobin, on the other hand, is a density or concentration measurement and is expressed in grams per liter or deciliter. (Hemoglobin is, if you will recall from your high school biology, the iron-based protein that transports oxygen.) RBC is a simple count and is usually expressed as the number of million red blood cells that you have per microliter. Usually, hematocrit is three times the amount of hemoglobin and can be measured through a simple blood sample test. What are the normal ranges for hematocrit? Normal levels of hematocrit for men range from 41% to 50%. normal level for women is 36% to 48%. Why does TRT increase hematocrit? Erythrocytosis is a medical condition that appears when the body makes too many red blood cells. RBCs are responsible for transporting oxygen to organs and tissues. When there are too many, the blood can become too thick and cause cardiovascular complications. There are two types of erythrocytosis: primary and secondary. Problems with the bone marrow, such as bone marrow disease, are typically the cause of primary erythrocytosis. RBCs are made in the bone marrow, and something might trigger an increase in their production. Certain diseases or medications, such as testosterone replacement therapy, can cause secondary erythrocytosis. Some studies concluded that testosterone reduces hepcidin (a hepatic hormone), which is related to iron absorption pathways. When hepcidin is reduced, erythrocytosis is increased [1] An increase in hemoglobin (Hb) and hematocrit (Hct) is indicative of this medical condition. When the Hb is higher than 18.5 g/dL and the Hct is higher than 52% in men, the patient suffers from erythrocytosis. What are the risks of high hematocrit? One of the primary risks of testosterone that you need to be aware of is called polycythemia or erythrocytosis. This is a condition where your body produces too many red blood cells, also known as high hematocrit levels or secondary polycythemia. Hematocrit refers to the percent of red blood cell content in your blood, also known as Hct levels. If your hemocrit levels rise, your blood will become too thick or viscous. This can, in turn, make it more likely that you will develop strokes, heart attacks, and clotting events. Polycythemia is serious and potentially life-threatening if untreated. Since the RBC count is too high in people with erythrocytosis, the blood viscosity also increases, which can lead to various potentially life-threatening medical issues such as venous thromboembolism. This essentially means that tiny blood clots separate from their original source and travel through veins and capillaries, causing blockages that result in stroke, myocardial infarction, or other complications related to reduced blood flow and blood volume. Individuals with high hematocrit levels may also be at risk for conditions such as polycythemia vera, a bone marrow disease that causes an abnormal increase in red blood cells and can lead to symptoms of polycythemia vera such as headache, dizziness, and fatigue. Other potential risks include congenital heart disease, exposure to high altitudes, and reactions to blood transfusions. It can be quite stressful for a man who has finally gotten on TRT, feels better, and then finds out that his hemoglobin is high. Of course, he can always lower his testosterone dosage to try to solve the problem, but this may not be a solution that either doctor or patient wants to pursue. Many men have found that their erectile dysfunction is greatly helped and/or morning erections and libido have returned. The last thing they want to do is lower their dose. So why even worry about a high hemoglobin or RBC count? What’s a few extra red blood cells anyway? Unfortunately, high hemoglobin (or RBCs) is a risk factor for ischemic stroke, i.e., the standard kind of stroke where there is a loss of blood supply to tissues such that permanent damage is usually incurred. [2] Of course, a stroke can be a life-changing (or life-ending) event and should be avoided at all costs. There is also a longer-term risk: elevated hemoglobin could lead to unhealthy iron store levels, which are associated with heart disease and dementia. Iron in tissues can lead to oxidative damage. Just look at what some recent studies have concluded: “Low and high hemoglobin concentrations in older persons are associated with a lower level of cognitive function in old age, particularly in semantic memory and perceptual speed.” [3] “In older persons without dementia, both lower and higher hemoglobin levels are associated with an increased hazard for developing AD [Alzheimer’s Disease] and more rapid cognitive decline.” [4] Can hematocrit stabilize in men on TRT? Hematocrit may stabilize after long-term testosterone replacement. Although there is only one study done in mice, it may explain why hematocrit may eventually decrease and stabilize in men on TRT. There seems to be an adaptive mechanism that makes red blood cell indices change while hematocrit stabilizes. In some men, red blood cell indices (MCV and MCHC) start changing after starting TRT as a way for the body to compensate for the extra production of red blood cells. There are three red blood cell indices: mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC). They are measured by a machine, and their values come from other measurements on a CBC panel. The MCV shows the size of the red blood cells. The MCH value is the amount of hemoglobin in an average red blood cell. The MCHC measures the concentration of hemoglobin in an average red blood cell. [5] Another study that followed frequent blood donors found a reduction in ferritin in them, created as a way for the body to increase iron absorption in the presence of lower hematocrit. Ferritin and hematocrit stabilized after five donations.[6] How to Lower High Hematocrit on TRT Some physicians and TRT guidelines believe that the best way to lower hematocrit is to stop TRT. But stopping TRT can have negative consequences in the quality of life, as men who do so tend to stay hypogonadal for months, and most do not return to “normal levels.”. Fortunately, there are several ways to decrease high hematocrit and also potentially prevent it from happening. Give Blood. This is a time-proven technique for men on testosterone therapy to lower their hemoglobin levels. And you are helping out someone else while you’re doing it! Every unit of blood donated can decrease hematocrit by 3 points, which is equivalent to one pint of blood. However, be careful not to donate more frequently than every 2.5 months, as the Red Cross advises, to prevent losing too much iron and ferritin, which can cause fatigue in men using testosterone therapy. You can check your iron and ferritin levels with this iron blood test. It's recommended that you donate when you are in the 51–52 hematocrit range. However, some organizations (like the Red Cross) will reject blood with a hematocrit higher than 53%, so it is good to avoid that high hematocrit level if you want to donate blood. Men who are rejected from blood donations because of high hematocrit can still give blood if their physicians call in an order for a therapeutic phlebotomy at the local blood center. Lower Your TRT Dose. If you have high hemoglobin or hematocrit from testosterone therapy, then your doctor may require you to lower your dose. This is not always a bad thing, as some men are actually taking more testosterone than they actually need, which can lead to side effects in both the long and short term. Drink Water. It is important to remember that hemoglobin is very dependent on your hydration levels. If you were dehydrated when you had your blood drawn, this could have made things worse. If you think you were dehydrated, discuss a retest with your doctor. Treat Thyroid Issues. Hypothyroidism (low thyroid function) can lower your RBC counts, and hyperthyroidism (high thyroid function) can raise them, too. If you haven’t checked your thyroid function lately, this might be wise. And don’t forget to get a full thyroid panel, including thyroid antibodies, if you can afford it. [10] Consider transdermal (topical) or oral testosterone. One research summary stated that topical testosterone creams or gels increase hematocrit, in general, less than intramuscular testosterone injections: “Intramuscular testosterone is the only form that significantly increases hematocrit above normal levels. However, it does so strongly, with up to a 6% change from baseline. The runner-up is testosterone gel, with an average increase of 2.5% over baseline levels.” [7]. Therefore, if you are on intramuscular injections and struggling with high hematocrit or hemoglobin, going on topicals may help a little. Discuss with your physician. NOTE: A cheap alternative is Compounded Testosterone Creams and Gels. Another emerging option is oral testosterone products. Switch from intramuscular injections to lower-dose subcutaneous Subcutaneous Testosterone Injections. Two hundred thirty-two men took part in a University of California study. Baseline levels were recorded for all men in each of the four measurement areas and then again at 6–12 weeks post-treatment. The results showed that men who underwent subcutaneous testosterone (SubQ) injections had a 14% greater increase in total testosterone levels compared to the testosterone levels of intramuscular testosterone injection (IM) patients. SubQ patients also had a 41% lower hematocrit post-therapy than IM patients and 26.5% lower estradiol levels. For both groups of men, there were no elevated levels of PSA. [7] Avoid or Reduce the Consumption of Red Meats. It is interesting because one of the criticisms that meat eaters level against vegetarians is that plant foods have many “anti-nutrients” that can slow down or bind with minerals such as iron. For example, organizations like Weston Price love to castigate vegetarians for their phytic acid consumption. Phytic acid is present in plant foods and binds to iron, magnesium, phosphorous, and calcium. It can, if overconsumed, lead to mineral deficiencies. However, Dr. Bernard points out that usually, it is likely very health-protective for most people because these minerals, as in the case of zinc and iron, are neurotoxic at even relatively low levels of tissue accumulation. Research has also shown that too much iron also contributes to heart disease, and there may be a link to colon cancer as well. [8]So, avoiding red meats, which are high in iron, stands a good chance of lowering your hemoglobin scores and protecting your long-term health unless some other preventative action is taken (such as giving blood). Actual dietary studies are required to support this statement. As a verification, one study of vegetarians and non-vegetarians found that females had significantly lower hemoglobin levels. Males had lower levels, but it may not have been statistically significant. [8] However, another study was more definitive and concluded: “It was found that hemoglobin, hematocrit, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, white blood cells, neutrophils, serum ferritin, and serum vitamin B12 in vegetarians were significantly lower than control subjects.” [11] Ferritin is a key measure, by the way, because it indicates that tissue levels of iron are lower and thus will likely cause less permanent damage. (This study did show that some vegetarians were iron deficient, as should be noted.) Fix Sleep Apnea. Sleep apnea can cause depleted oxygen saturation values that can enhance the body's ability to produce more red blood cells and hemoglobin as a way to compensate for the low blood levels of oxygen during the sleep cycle. And, sure enough, there are studies that confirm this as well. [12] So, if your hematocrit, hemoglobin, or RBCs are running high, think about getting tested for sleep apnea. A recent study commented that “one possible explanation is that repeated episodes of nocturnal hypoxia (low oxygen condition) lead to a hypercoagulable state that predisposes patients to thrombotic (blood clotting) events. There is evidence supporting a wide array of hematological changes that affect hemostasis (e.g., increased hematocrit, blood viscosity, platelet activation, clotting factors, and decreased fibrinolytic activity).” Reduce Inflammation. Hepcidin, the iron absorption-modulating hormone, can be decreased even further by inflammation. Checking for infections, CRP levels, etc., and then treating the underlying cause may help. [13] Consider Curcumin (Turmeric). Turmeric or curcumin, is increasingly studied as an anti-inflammatory and anti-cancer agent. It binds to ferric iron in the gut and causes iron deficiency in mice. A case history reported a possible case of iron deficiency anemia in a human taking turmeric. [14] Stop Smoking. Smoking reduces the amount of oxygen in the blood and makes the body produce more red blood cells and hemoglobin to compensate for that lower oxygen saturation.[14] Treat High Blood Pressure with Losartan. If you have high blood pressure, consider taking Losartan.[15] Losartan can be safely and effectively used to normalize hematocrit in patients with COPD and erythrocytosis, an effect that could obviate the need for therapeutic phlebotomy. Consider Grapefruit. Grapefruit extract (narigin) may decrease hematocrit [16]. There was no significant difference between ingesting 1/2 or 1 grapefruit per day, but a decrease in hematocrit due to ingestion of grapefruit was statistically significant at the p less than 0.01 level. However, discuss with your physician the fact that grapefruit can increase the blood levels of medications. The most important message of this article is that monitoring hematocrit every few months is a smart way to minimize cardiovascular risks associated with high hematocrit. You can buy your hematocrit and related tests on DiscountedLabs.com at affordable prices. Hematocrit is included in the CBC and other panels on Discounted Labs: Get Your Hematocrit Test Now Testosterone, Hematocrit, Ultrasensitive Estradiol and Prolactin Panel Hematocrit + Total and Free Testosterone References The Journal of Clinical Endocrinology & Metabolism, Volume 95, Issue 10, 1 October 2010, Pages 4743–4747 Eur Neurol, 1996, 36(2):85-8. Neuroepidemiology, 2008 December, 32(1): 40 46, “ Relation of Hemoglobin to Level of Cognitive Function in Older Persons” Neurology, 2011 Jul 19, 77(3):219-26, “Hemoglobin level in older persons and incident Alzheimer disease: prospective cohort analysis. Endocrinology. 2015 May; 156(5): 1623–1629. TRANSFUSION 2008; 48: 2197-2204. Comparison of Outcomes for Hypogonadal Men Treated with Intramuscular Testosterone Cypionate versus Subcutaneous Testosterone Enanthate SIU Academy. Choi E. 10/10/20; 309864; BSP-06.01 International Journal of Natural and Applied Sciences Vol. 2 (3) 2006: pp. 174–177, “Comparative study of the hemoglobin concentration of vegetarian and non-vegetarian subjects in Ogun state, Nigeria” World J Gastroenterol, 2006 September 21, 12(35): 5644-5650, “Hemoglobin induces colon cancer cell proliferation by release of reactive oxygen species” Iran J Ped Hematol Oncol, 2013; 3(2):73-77, “Effect of Thyroid Dysfunctions on Blood Cell Count and Red Blood Cell Indices” J Med Assoc Thai, 1999 Mar, 82(3):304-11, “Hematological parameters, ferritin and vitamin B12 in vegetarians” Can Respir J. 2011 Nov-Dec; 18(6): 338-348, “Coagulability in obstructive sleep apnea” Am J Kidney Dis. 2012;59(3):444-451 -
How to Stop TRT with Post Cycle Therapy (PCT)
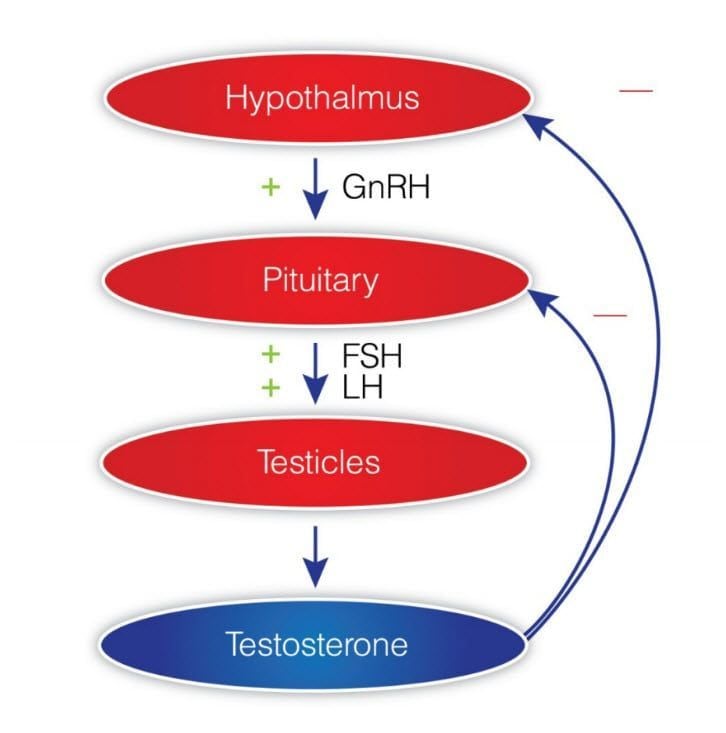
Categories: Testosterone Tests , Testosterone Side Effect Management , TRT Side Effects , Testosterone Blood Tests , Testosterone Lab Tests , LH Lab Test , FSH Fertility Test , Bodybuilder lab testsHow to Safely Use PCT After TRT: Stopping Testosterone Replacement Therapy Table of Contents What is Post Cycle Therapy PCT? Why Do Men Stop TRT? Common reasons a man may need to discontinue TRT include: Normalizing Natural Testosterone After Stopping TRT PCT Treatments to Jump Start Natural Testosterone and Sperm Production How to Know if Your PCT Worked? Buy Discounted Lab's Post-PCT Panel References: There is a common phrase most men will hear when they consider testosterone replacement therapy (TRT); it may be something they hear from friends or often what they read online: "TRT is for life." There is an element of truth to this statement: when a man has low testosterone, in order to treat it and maintain healthy or optimal levels, he will always need TRT to achieve it. However, saying "it's for life" remains a somewhat inaccurate statement, and this is where we enter into the realm of what is commonly referred to as Post Cycle Therapy or PCT. TRT and anabolic androgenic steroids (AAS) can lead to dysfunction in HPTA (Hypothalamic-Pituitary-Testicular Axis). Supplemental testosterone can inhibit the release of the body's own testosterone production through negative feedback inhibition on LH levels. This feedback inhibition also results in the suppression of FSH levels, leading to the suppression of sperm production (spermatogenesis). During recent years a large surge in testosterone prescriptions and TRT clinics has unfortunately led to many men who have been misdiagnosed with low testosterone yet placed on TRT when it may not have been needed in the first place. If you are one of these men and you are considering discontinuing testosterone treatments, some protocols can help restore your hormone axis. You do not want to stop testosterone "cold turkey," which will lead to unnecessary symptoms that could last for many months. Understanding TRT and Its Impact on the Body Testosterone Replacement Therapy (TRT) can be a game-changer for men with low testosterone levels, but it's crucial to understand how it impacts the body. TRT involves introducing exogenous testosterone into the body, which can disrupt the natural hormone production process. To grasp the full picture, we need to explore the Hypothalamic-Pituitary-Testicular Axis (HPTA) and how TRT affects it. The Hypothalamic-Pituitary-Testicular Axis and TRT The Hypothalamic-Pituitary-Testicular Axis (HPTA) is a sophisticated system that regulates testosterone production. It starts with the hypothalamus, which produces Gonadotropin-Releasing Hormone (GnRH). This hormone signals the pituitary gland to release Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH). LH and FSH then stimulate the testes to produce testosterone. When you undergo Testosterone Replacement Therapy (TRT), this delicate balance can be disrupted. The introduction of exogenous testosterone can suppress the body's natural production of LH and FSH, leading to a decrease in the body's ability to produce testosterone on its own. Impact of TRT on Natural Testosterone Production The impact of TRT on natural testosterone production can be significant. When exogenous testosterone is introduced, it can lead to a suppression of LH and FSH, which are crucial for natural testosterone production. This suppression can result in various symptoms, such as low libido, fatigue, and decreased muscle mass. Over time, prolonged use of TRT can lead to hypogonadism, a condition where the testes are unable to produce sufficient testosterone. This is why understanding the effects of TRT on natural hormone production is essential for anyone considering or currently undergoing TRT. What is Post Cycle Therapy PCT? PCT is a treatment plan after discontinuing anabolic androgenic steroids (AAS). It is a phrase most commonly associated with what we might call "recreational steroid users" (RSU), such as bodybuilders: people who do not need steroid hormones like testosterone for medical reasons but use them for muscular competition advantage. In such cases, the individual will supplement with AAS for a set period of time, known as a steroid cycle, and then discontinue use. As his use of AAS shut down his natural testosterone production, just as it does with TRT, he will often implement a PCT plan for natural production to restart. Such plans will include Selective Estrogen Receptor Modulators (SERMs) or other items, such as the peptide HCG. The goal for the RSU, as eluded to prior, is to regain his natural production of testosterone as quickly and efficiently as possible. There is no guarantee this will work. There is no guarantee he will reach his previous levels before AAS use, although perhaps levels that accurate enough. Then we have the TRT patient; such an individual had low testosterone levels before he began administering exogenous testosterone. The use of testosterone, just as it did with the RSU, will stop his natural production. This is a factor that bothers many men, but let us keep in mind a very significant one: you already had low levels, your body was not able to produce enough, to begin with, and was not going to be able to, or you wouldn't be on TRT. Nonetheless, there are reasons some men may find they need to discontinue use, and when that occurs, a PCT plan may be in order. Such a plan will not address his primary issue, low testosterone, but the goal here is to get at least some natural production back online. Why Do Men Stop Testosterone Replacement Therapy? Common reasons a man may need to discontinue TRT include: Need for Fertility TRT Cost TRT Side Effects or Health Issues Of the three potential reasons to stop TRT, fertility is the overwhelming reason for most men. Along with suppressing natural testosterone production, TRT can also have a negative impact on sperm production. There was a time in history not that long ago when it was thought exogenous testosterone would be touted as a male contraceptive. This idea died out when many men using testosterone found they were still able to impregnate a female. While many men on testosterone were found to be severely lacking in this department, it wasn't enough or significant enough to market the hormone as an actual contraceptive. The other common reasons for discontinuing TRT are cost and side effects. These are the least common reasons in comparison to fertility needs or desires, but both are still possible. We all go through points in life where money can get a little tight; loss of a job, unexpected expenses – whatever the reason, if you find you need to stop, considering a PCT plan with your physician will make the transition easier. You're still going to have low testosterone levels in the end – remember, you already had them, or you wouldn't have started TRT in the first place – but you'll hopefully be in a better position than you would be without, and in time, when your situation improves, you'll be able to jump back on your TRT plan. The same may hold true for the individual who has side effect issues. This will be the least common reason for discontinuation of TRT but certainly within the realm of possibility. You could be one of the rare individuals who cannot control his hematocrit even with regular therapeutic phlebotomy. You could be someone that has other health concerns and, for whatever reason, need to discontinue use until you figure out what's going on with your body. Hormonal imbalances, such as elevated estrogen levels, can also occur when stopping TRT, leading to conditions like gynecomastia. As was with the individual who was experiencing income issues, a PCT plan may be in order. Preparing for TRT Discontinuation Deciding to discontinue TRT is a significant step and should be approached with caution. One of the most critical aspects of stopping TRT safely is to do so under the guidance of a medical professional. Abruptly stopping TRT can lead to severe withdrawal symptoms and a dramatic drop in testosterone levels, which can be detrimental to your health. Gradual Tapering Under Medical Supervision When it comes to discontinuing TRT, gradual tapering is the safest approach. This process involves slowly reducing the dosage and frequency of testosterone administration to allow the body to adjust and begin producing testosterone naturally again. A healthcare provider can create a personalized tapering schedule based on factors such as the dosage and duration of your TRT use. This might involve reducing the amount of testosterone you inject or apply through gels over a set period. Regular check-ups with your healthcare provider are crucial during this time to monitor your progress and make any necessary adjustments to your tapering plan. This careful and monitored approach helps minimize withdrawal symptoms and supports the body's natural transition back to producing testosterone on its own. By understanding the impact of TRT on your body and following a medically supervised tapering plan, you can safely discontinue TRT and support your body's return to natural testosterone production. Normalizing Natural Testosterone After Stopping TRT For most men, studies have shown that for men who stop TRT, natural testosterone production can normalize within three months or longer, and spermiogenesis in well over a year. This is certainly not optimal when conception is the goal, which leads to the possible need for a PCT protocol. Post cycle therapy (PCT) is crucial in maintaining and recovering natural testosterone levels after using performance-enhancing drugs, as it helps enhance the body's own testosterone production. PCT Treatments to Restore Hormonal Balance and Jump Start Natural Testosterone and Sperm Production The use of the SERMs has been shown to increase testosterone levels to baseline in as little as 2-4 weeks. Studies have also shown spermiogenesis to improve significantly within 3-6 months. Clomid as we can easily see, greatly improves the time frames of recovery of these two important factors related to conceiving (testosterone and semen). PCT is crucial to restore hormonal balance, helping individuals recover from the use of anabolic steroids by promoting natural testosterone production and mitigating adverse effects caused by hormonal imbalances. HCG is another item commonly used in PCT for fertility purposes. HCG PCT has the ability to stimulate both testosterone production and spermiogenesis. It is not uncommon for fertility specialists to try both Clomid and HCG and, in some cases, in conjunction with one another. Unfortunately, there is much controversy among many fertility specialists regarding how much HCG should be administered for this purpose. While many physicians will prescribe SERMs in the range of 25-50mg per day to every other day, commonly prescribed HCG doses can run anywhere from 1000iu per day to 2500iu or even larger doses split into every other day schedules. Other common drugs used in this treatment, but to a lesser extent, include the SERM Tamoxifen Citrate, best known by its most notable trade name, Nolvadex. Treatments usually requires 4 weeks. Unfortunately, for some men, a PCT plan that includes some or all of these medications will not work. A HCG PCT plan is most likely to work in a TRT patient who is receiving treatment due to secondary hypogonadism. If a PCT plan has not worked – testosterone levels and sperm count have not increased – it is likely that the individual has primary hypogonadism, and as a result, will be best served (quality of life) by remaining on TRT. It's imperative to note: this individual had primary hypogonadism prior to beginning TRT, he did not obtain it because of TRT. How to Know if Your PCT Worked? After going through PCT, physicians tend to check your testosterone blood levels and upstream hormones like LH and FSH to determine if your hormone axis has been restored. Discounted Labs has created a Post PCT Lab Test Panel that makes it easy for men to know if their PCT has successfully worked. This lab test panel is designed to measure the health and recovery of the Hypothalamic-Pituitary-Testicular Axis (HPTA) after attempting to normalize it spontaneously or with the use of Post Cycle Therapy (PCT) (with the use of clomiphene, hCG, and other treatments) It is suggested that this panel be done no sooner than 4 weeks after PCT cessation and in a fasting state. You should fast for 12 hours before collection of the specimen. Fasting is defined as no consumption of food or beverage other than water for at least 12 hours before testing. If using a testosterone cream please be sure you have not rubbed any into the antecubital area of your arm for the last 24 hours as it can give elevated results. Lab tests included in the post-PCTest Panel: Ultra Sensitive Estradiol Test by Liquid Chromatography/Mass Spectrometry (LC/MS assay used to measure estradiol in men more accurately estradiol in men) Total and Free Testosterone LC/MS- No upper limit Luteinizing Hormone (LH) (responsible for activating Leydig testicular cells to produce your own testosterone). This hormone is shut down by testosterone replacement or AAS. Follicle Stimulating Hormone (FSH) (Responsible for activating Sertoli testicular cells to produce sperm). This hormone is shut down by testosterone replacement or AAS. CBC - Complete Blood Count (Includes hematocrit- red blood cell volume) CMP - Comprehensive Metabolic Panel (Includes liver and kidney function, glucose and electrolytes) For any man, simply discontinuing the use of testosterone can be difficult, to put it mildly. Your testosterone levels will completely bottom out when going the cold-turkey route, and this often. This severe sexual dysfunction, decreased energy, and even depression, to name a few of the consequences. Your levels may go up enough to at least function, to a degree, but it's going to take an enormous amount of time, as previously discussed. Cutting this time down significantly, and giving your body a boost in testosterone during the therapy process, is the only means of discontinuation that makes any sense, meaning some form of a PCT plan is a sensible approach. Buy Discounted Lab's Post-PCT Panel References: Diagnosis and Management of Anabolic Androgenic Steroid Use Testosterone Use in the Male Infertility Population: Prescribing Patterns and Effects on Semen and Hormonal Parameters How to Stop TRT Safely -

Why Do I Feel So Tired After Testosterone ?
Categories: Testosterone Tests , Testosterone Side Effect Management , TRT Side Effects , Estradiol Estrogen Tests for Men , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , TRT Testing , TRT Monitoring , Testosterone Replacement Monitoring Tests , Free Testosterone Test , Fatigue Blood TestsCan Testosterone Make You Tired? Some men start testosterone replacement therapy (TRT) to address low T and testosterone deficiency and find out their baseline fatigue and low energy get worse. Testosterone and Energy Levels Testosterone controls energy levels in men. When testosterone is within normal range, men feel more energetic and motivated. Testosterone supplementation can also help restore energy in men with low testosterone. Low testosterone can cause fatigue, lethargy, and feeling unwell. Testosterone helps regulate the body’s metabolism, which converts food into energy. Studies have shown that testosterone levels are related to energy levels. Men with low testosterone have lower energy levels; men with normal or high testosterone have higher energy levels. Testosterone replacement therapy also helps improve energy in men with low testosterone. By getting testosterone levels back to normal range, many men feel a big boost in overall energy and vitality. Why does TRT cause fatigue? TRT can cause fatigue in some men for the following reasons: Overstimulation of the body: Increased testosterone can overwork the body and cause fatigue and exhaustion. Insomnia: Some men on testosterone therapy may have difficulty sleeping and get fatigue. Hormonal imbalance: Sudden increase in testosterone can cause imbalance with other hormones in the body and cause fatigue and other symptoms. Side effects of the medication: Testosterone medication can cause side effects like acne, fluid retention, and mood changes, which can also cause fatigue. Testosterone injections, which are a common method of TRT, can cause these side effects. As testosterone levels drop, men may feel more fatigue and lower energy levels, which can be worsened by TRT. Note that testosterone therapy can also help improve energy and reduce fatigue in some men but it’s best to discuss the benefits and risks with a healthcare provider before starting treatment. If no improvement in fatigue is seen after 6 weeks of testosterone replacement, other factors beyond hypogonadism may be present. This article will review a few ways to find out what causes TRT fatigue. Low Testosterone Symptoms Low testosterone can cause many testosterone deficiency symptoms, including: Fatigue and lethargy Low sex drive Erectile dysfunction Loss of muscle mass and strength Increased body fat Decreased bone density Mood changes like depression and anxiety Difficulty concentrating and memory problems If you have any of these symptoms, consult a healthcare professional to find out if low testosterone is the cause. A proper diagnosis will help you explore treatment options, including testosterone replacement therapy, to alleviate these symptoms and improve your life. Thyroid Function and Hormonal Imbalance: The thyroid is a butterfly-shaped endocrine gland located in the lower front of the neck. It produces thyroxine or T4, which is converted to triiodothyronine or T3. T4 production is controlled by thyroid-stimulating hormone or TSH, which is produced by the pituitary. Hypothyroidism, or low thyroid hormone production, can cause sexual dysfunction and depression, fatigue, dry skin and hair, weight gain, and increased sensitivity to cold. Blood tests to measure TSH, T4, and T3 are available and widely used. The American Thyroid Association (thyroid.org) has great info on how to find out if you have hypothyroidism that’s causing your fatigue. Testosterone can decrease thyroxin-binding globulin and total T4 serum levels and increase resin uptake of T3 and T4. Free thyroid hormone levels remain the same and there’s no clinical evidence of thyroid dysfunction. Once thyroid hormone levels are normalized, testosterone tends to increase naturally. Check your thyroid hormones here: Choose Your Test | Discounted Labs Adrenal Function and Chronic Fatigue: The adrenal glands are located in the abdomen above the kidneys and regulate stress in the human body. When the body is in an emergency situation, the adrenal glands release hormones like adrenaline to enable the body to respond. You may have experienced this reaction called the “fight or flight” response if you were in danger, fear, or shock. Adrenal fatigue is the controversial idea that the adrenal glands can get worn out and cause illness if continuously overstimulated. Proponents of the “adrenal fatigue” theory believe that the adrenal glands may be overworked in some individuals and therefore get “fatigued” and unable to produce enough hormones. When your adrenal glands are exhausted, your cortisol levels drop significantly. Cortisol is your natural stress hormone. Low sex drive and infertility are symptoms of adrenal fatigue. Other symptoms include chronic fatigue, low blood pressure and low blood sugar, dizziness, headaches, anxiety or panic attacks, depression, and other equally debilitating problems. Some doctors may prescribe low doses of corticosteroids if your morning cortisol levels (measured by blood, saliva, or urine tests) are low. But be careful with corticosteroids, as they can increase fat mass and decrease bone density if given in doses higher than what the healthy adrenals would produce. Check your adrenal health. DHEA and Testosterone Levels: The adrenal glands also produce dehydroepiandrosterone (DHEA), the most abundant hormone in the bloodstream. The body uses DHEA as the starting material to produce the sex hormones testosterone and estrogen in men. DHEA supplementation can increase DHEA levels, which in turn can support testosterone production. Studies show it only increases testosterone in women. DHEA production decreases in most people after age 40. In people 70 years old, DHEA levels will be 30% lower than what they were at age 25. Low DHEA levels are associated with many degenerative conditions. Some studies are controversial and inconclusive that people with immune deficiencies and fatigue may benefit from supplementation with this hormone. It’s still available over-the-counter in the US. This may change soon, as a new bill was passed by Congress classifying it as a performance-enhancing steroid (no studies show it has such an effect). One study showed that women with normal DHEA levels can convert it into testosterone as their body needs while men don’t benefit the same way. You need a blood test to know if you have low DHEA-S since most of the DHEA converts into this sulfated form. Common doses for women are 5-30 mg a day, while men benefit from 25-100 mg a day (to bring low DHEA-S to normal). NOTE: Do not use DHEA supplements unless your blood levels of DHEA-S are low. If low, start at a low dose and get your DHEA-S tested again after a month. Men who use DHEA supplements may have problems with higher estrogen levels since DHEA can also convert into estradiol. This can cause gynecomastia and water retention. If you start taking DHEA, get your blood levels checked to make sure they are not above normal. There are many claims about DHEA being an anti-aging and anti-cancer cure but none of these claims have been proven with strong data. To make diagnosis easier, we have created this new Fatigue Panel on DiscountedLabs.com at a discount. Click here: Comprehensive Fatigue Panel Sleep Apnea: Sleep apnea is a sleep disorder in which a person stops breathing or breathes shallowly many times during sleep and therefore doesn’t get enough restful sleep; oxygen levels in the blood drop and the brain starves of oxygen. Besides causing daytime fatigue, it can increase blood pressure and cardiovascular risks. Testosterone replacement therapy has been linked to the worsening of sleep apnea or the development of sleep apnea, especially in men who use higher doses of testosterone or who have other risk factors for sleep apnea (high body weight, thick necks, snoring, alcohol consumption, etc.). Upper-airway narrowing doesn’t seem to be caused by testosterone replacement therapy; it suggests that testosterone replacement contributes to sleep-disordered breathing by central mechanisms rather than by anatomical changes in the airway. Tell your doctor if your spouse or partner complains that you snore loudly at night and feel fatigued. The only way to know for sure if you have sleep apnea is to have your doctor refer you to a sleep lab for a sleep study. If you are diagnosed with sleep apnea, a continuous positive airway pressure (CPAP) machine can be prescribed to help open up your airways with a small air pump while you sleep. Some people love it; some hate wearing a mask while being hooked up to a machine at night. I have seen men regain their quality of life after starting CPAP. It’s covered by insurance, Medicare, and most HMOs. A new option for those who hate CPAP machines with mild to moderate apnea is the use of oral appliances. Worn in the mouth like an orthodontic appliance during sleep, oral appliances keep the soft tissue from collapsing and interrupting normal breathing patterns. The purpose of the oral appliance may be to reposition the lower jaw, tongue, soft palate, and hyoid bone into a certain position; to keep the airway open with stabilization of the tongue and jaw; or to provide artificial muscle tone to prevent collapse and resulting airway blockage. The doctors will fit your oral appliance for comfort by using a mold of your mouth to design your unique fit. Fatigue Management with Testosterone Therapy Testosterone therapy can help manage fatigue in men with low testosterone. Testosterone gel is another way to get testosterone therapy to help manage fatigue. Testosterone therapy can bring many health benefits, including improved cardiovascular health, better blood sugar control and reduced risk of osteoporosis and diabetes. But it’s important to understand the benefits and risks of testosterone therapy and to discuss them with your doctor. Some men will experience a big boost in energy and overall well-being; others will find their fatigue persists or even worsens. This variability is why personalized medical advice and regular monitoring are important to tailor the treatment to your needs. Energy Tips In addition to testosterone therapy, there are several lifestyle changes that can help men regain energy and overall health. These are: Regular Exercise: Strength training and cardio exercises can help build muscle and boost energy. Exercise also helps with better sleep and reduces stress, which can further increase energy. Healthy Diet: Eating a balanced diet rich in protein, healthy fats, and complex carbohydrates can give you energy all day. Lean meats, fish, nuts, seeds, and whole grains are good choices. Sleep: Aim for 7-9 hours of sleep per night to help regulate testosterone and energy. Good sleep hygiene practices like a consistent sleep schedule and a restful environment can make a big difference. Stress Management: Meditation, yoga, or deep breathing exercises can help manage stress, which can help increase energy. Chronic stress can lower testosterone so finding ways to cope is important. Hydration: Drinking plenty of water throughout the day is key to maintaining energy and overall health. Dehydration can cause fatigue and decreased physical performance. Natural Testosterone Boosters While testosterone replacement therapy may be needed for some men, there are also natural testosterone boosters that can increase testosterone. These are: Exercise Regularly: Exercise, especially weightlifting and high-intensity interval training, can increase testosterone. Eat a Healthy Diet: A diet rich in protein, healthy fats, and complex carbohydrates can support testosterone. Get Enough Sleep: Sleep is key to testosterone production so aim for 7-9 hours of sleep per night. Reduce Stress: High stress can lower testosterone so find ways to manage stress through meditation or yoga. Get Enough Vitamin D: D: Vitamin D is important for testosterone production, so make sure you get enough through sun exposure, supplements, or fortified foods. Implementing these lifestyle changes can support your body’s natural testosterone production, and if you’re already on testosterone replacement therapy,. Testosterone Therapy Risks and Considerations Testosterone therapy can be good for men with low testosterone, but there are testosterone side effects and considerations to be aware of: Blood Clots and Stroke: Testosterone therapy can increase the risk of blood clots, which can cause stroke or other cardiovascular events. Cholesterol and Cardiovascular Health: Testosterone therapy can affect cholesterol levels, which can increase heart disease risk. Lipid profiles should be monitored regularly. Fertility and Sperm Production: Testosterone therapy can reduce sperm production. Men who want to have children should talk to their doctor. What to Expect from Testosterone Men on testosterone therapy can expect: Increased Energy and Reduced Fatigue: Many men feel more energetic and less fatigued after starting testosterone therapy. More Muscle and Strength: Testosterone therapy can increase muscle mass and strength for better physical performance and overall health. Better Bone Density: Testosterone therapy can increase bone density, reducing the risk of osteoporosis and fractures. Libido and Sexual Function: Many men experience improved libido and sexual function, which can improve their quality of life. Overall Well-Being: Testosterone therapy can improve mood and overall sense of well-being for better quality of life. But you need to have realistic expectations and understand that testosterone therapy is not a magic pill. It may take several months to see the full effects and regular monitoring and adjustments may be needed to get the best results. Testosterone Monitoring Monitoring testosterone levels is crucial to ensure treatment is working and to minimize side effects. This means working with a healthcare professional to track progress and adjust therapy. Why Blood Tests Blood work is needed to monitor testosterone levels and adjust treatment. These tests can: Confirm Diagnosis: Blood tests can confirm low testosterone levels so testosterone therapy is appropriate. Monitor Results: Testing helps to monitor testosterone therapy and ensure testosterone levels are in range. Identify Side Effects: Blood tests can detect side effects like changes in cholesterol or liver function so treatment can be adjusted. Healthy Ranges: Keeping testosterone levels in a healthy range is key to minimizing risk and maximizing benefits. You need to work with a healthcare professional to determine the best testing schedule and to make sure testosterone levels are being monitored regularly. This proactive approach will get the best results and overall health. Get your own testosterone test here. When to See a Doctor for Fatigue If you have persistent or severe fatigue, you need to see a doctor. Fatigue can be a sign of an underlying medical condition like low testosterone, anemia, or diabetes. A healthcare professional can help figure out what’s causing your fatigue and develop a plan to treat it. If you have any of the following, see a doctor: Fatigue that lasts more than 2 weeks Severe fatigue that affects daily activities Fatigue with other symptoms like weight loss, fever, or night sweats Fatigue that doesn’t go away with rest or sleep A healthcare professional can do a physical exam, take a medical history and order diagnostic tests like blood work to figure out what’s causing your fatigue. Knowing the cause is key to developing a treatment plan and overall health and wellness. References Here are the clickable links with their corresponding titles: Can Testosterone Replacement Therapy Cause Insomnia? TRT and Fatigue: Understanding the Connection and How to Overcome It Testosterone Therapy: Effects and What to Expect Experiencing Extreme Tiredness and Fatigue on TRT? Can Testosterone Therapy Make Me Less Tired? Addressing Fatigue with Testosterone Pellets -
Do You Need to Fast for a Testosterone Test?
Categories: Testosterone Tests , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , Bodybuilder lab tests , Fasting blood testsHow Long to Fast Before a Testosterone Blood Test: Do You Need To? About 5 million American men suffer from low testosterone levels. This is also known as hypogonadism and can have significant effects on your life. Hypogonadism (testosterone deficiency) is diagnosed by running multiple tests. Patients get one or more testosterone tests to measure their levels. But recent studies found out that your testosterone levels can be affected if the tests were done while fasting. In other words, having a meal before a testosterone test can change the results. Read on to find out more about the correlation between testosterone levels and fasting. How to Test for Low Testosterone? What is the correlation between fasting and testosterone? Study 1 - Testosterone went down significantly after an oral glucose load Study 2 - Eating a meal can lower testosterone levels by a lot Key Takeaway for Future Testosterone Testing Protocols About 5 million American men suffer from low testosterone levels. This is also known as hypogonadism and can have significant effects on your life. Hypogonadism (testosterone deficiency) is diagnosed by running multiple tests. Patients get one or more testosterone tests to measure their levels. But recent studies found out that your testosterone levels can be affected if the tests were done while fasting. In other words, having a meal before a testosterone test can change the results. Read on to find out more. What is a Testosterone Test? A testosterone test is a medical test to measure the level of testosterone in your blood. Testosterone is a hormone produced by the adrenal glands and gonads (ovaries in females and testes in males) that is important for the development and maintenance of male reproductive tissues, bone density and muscle mass. In females, testosterone is present in smaller amounts and helps in the growth and development of bones and muscles. Why is a Testosterone Test Performed? A testosterone test is performed to diagnose and monitor various medical conditions related to abnormal testosterone levels. The test can help identify: Testosterone Deficiency (Hypogonadism): In males, low testosterone levels can cause low sex drive, fatigue, and decreased muscle mass. Testosterone Excess (Hyperandrogenism): In females, high testosterone levels can cause excessive hair growth, acne, and irregular menstrual cycles. Polycystic Ovary Syndrome (PCOS): This common endocrine disorder in females is characterized by high testosterone and androgen excess. Adrenal Gland Disorders: Conditions like Cushing's syndrome can cause abnormal testosterone production. Monitoring Therapy: It's also used to monitor testosterone levels in individuals undergoing testosterone replacement therapy or androgen deprivation therapy. Preparing for a Testosterone Test To prepare for a testosterone test: Schedule the Test in the Morning: Testosterone levels are highest in the morning, so schedule your test early in the day. Fasting Requirements: Fasting requirements vary by test type. Some testosterone tests require fasting for 12 hours, while others require no fasting at all. Check with your healthcare provider or testing facility for specific requirements for your test. Inform Your Doctor: Tell your doctor about any medications or supplements you are taking, as they may affect testosterone levels. Wear Comfortable Clothes: Wear loose and comfortable clothes and avoid tight sleeves that may make it hard to draw blood. Plan Your Visit: You will be at the testing facility for about 30 minutes, but the blood draw will only take a few minutes. By doing these you can get the most accurate testosterone test results. How to Diagnose Low Testosterone? Testosterone levels are highest in the morning for all healthy males. They start to drop after 11 am and continue to drop towards the end of the day. Testosterone tests are done in the morning because that's when the levels are highest. If a person sees the classic signs of low testosterone, a test might be required to check this out. These signs are low sex drive, poor concentration, fatigue and even depressive symptoms. But multiple tests are needed to confirm if the person is hypogonadal or not. A testosterone levels test measures the amount of testosterone in a blood sample. For example, your doctor might check your FSH and LH levels. These hormones are produced by the pituitary gland and trigger the testosterone and sperm production in the testicles. Depending on the lab, a healthy male should have a testosterone measurement between 350 ng/dl and 1,250 ng/dL. If below 350 ng/dl and you have low testosterone symptoms, you might be considered hypogonadal. Testosterone levels vary depending on the time of day, diet, age, fitness level and other factors. As mentioned earlier, testosterone tests are done in the morning when testosterone is at its peak. Fasting requirements vary by specific test type - some testosterone tests require fasting while others do not. But some studies suggest that fasting before a testosterone test can affect the results. What's the connection between Fasting and Testosterone Levels? In simple terms, fasting means not eating for a certain period of time, usually 8 to 12 hours. This also includes not drinking anything that makes your organs work to process them, like drinks, milk, etc. Many blood tests require patients to fast before drawing a sample. A standard glucose test is a good example of this. If you eat something and then do a glucose test, you might be labeled as diabetic. That's because your body didn't get a chance to process the glucose in your blood, and it will show up in the test. Scientists believe that fasting is also important when testing testosterone through blood tests. In short, eating before your test will temporarily lower your testosterone levels. This can lead to a false diagnosis of hypogonadism if your normal T level is around 400-500 ng/dL. Such findings also mean retesting subjects who were initially diagnosed with low testosterone. Let's look at a few studies and see the correlation between fasting and testosterone tests in more detail. You'll see how a glucose load or a full meal can affect the total and bioavailable testosterone levels hours after ingestion. Study 1 - Testosterone Decreased Significantly After an Oral Glucose Load This study was done on 74 men. The average age of the participants was around 50, give or take a few years. The study was done in 2012, and it was a standard 75-g oral glucose tolerance test. An oral glucose tolerance test measures how well your body can process glucose in the blood after you drink a sweet drink they give you at the lab. If you process it fast, your glucose tolerance is good. If it takes too long to process, it's usually associated with diabetes or other health problems. Almost 60% of the men in the study had normal glucose tolerance. More than 10% were newly diagnosed with diabetes, and about 30% had impaired glucose tolerance. Blood was drawn from each participant at the start of the study and at 30, 60, 90, and 120 minutes, respectively. Other hormones and substances were also measured, such as insulin, leptin, sex hormone-binding globulin (SHBG), and total testosterone levels. None of these individuals had low testosterone at the start of the study. But the results were surprising. The study showed that testosterone levels decreased by 25% after glucose ingestion. That's a big drop considering most of the participants had normal glucose tolerance. To put it into perspective, if an individual starts with an average testosterone level of 500 ng/dl, a 25% decrease would bring him down to 375 ng/dl. That's close to the bottom of the normal testosterone range. Interestingly, the testosterone suppression was still present after 120 minutes when blood samples were drawn for the last time. 10 of the participants could qualify for hypogonadism at the end of the study as their testosterone levels went below the baseline. This study shows how important it is to consider fasting status when interpreting testosterone test results. A simple glucose load can lower total testosterone levels and qualify someone for hypogonadism. Study 2 - Eating a Meal Can Decrease Testosterone Levels Let's look at another study that shows the correlation between testosterone levels and fed or fasting state. This study shows how a 550-calorie meal of protein, fat and carbohydrates can affect testosterone levels. 11 healthy men participated in this study. They were non-smokers, had no medical treatment, and had normal BMI. The average age was 43 years, and they had no significant medical history. In the first part of the study, the participants were given a 550-calorie meal of buttermilk, cheese, ham, orange juice, and other foods. Blood was drawn at various intervals. The study also measured other hormones such as LH, SHBG, and glucose. Free testosterone, the unbound fraction and biologically active, was also measured. The participants finished the meal in about 15 minutes. The foods were varied, as the study designers wanted to mimic a meal that most men would eat on a daily basis. Before the meal, the participants were told to fast for 12 hours. They were also instructed not to have sex or do any strenuous exercise that would affect their testosterone levels. The same procedure was repeated a few weeks later with the same participants. This time they only fasted for 12 hours and didn't eat after. Blood was drawn in the fasting state, and all other parameters were the same. When the two experiments were compared, the results were striking. In both groups, the initial fasting testosterone levels were the same. LH and SHBG were unchanged. But in the fed group, testosterone levels decreased 15 minutes after meal ingestion. And 30 minutes after the meal. Other hormones and parameters were the same; just total and bioavailable testosterone levels went down. Upon reviewing the results, the experts found out that the decrease in testosterone was 30%. This was true for all participants with no exceptions. This study shows how testing for testosterone in a fasted state is different from testing in a fed state. Takeaway for Future Testosterone Testing Protocols The scientific literature on sexual medicine says that food intake can affect testosterone levels. However, testosterone test protocols vary - some require fasting while others do not. The studies above highlight the importance of understanding how food intake can affect testosterone measurements and following the specific instructions for your particular test. Also, there was no significant difference in LH, SHBG, and other hormones among the participants. This means the hypothalamic-pituitary-testicular (HPT) axis was not really affected by food or glucose intake, but testosterone production was. It's believed that insulin, a hormone produced by the pancreas when we eat to process glucose, can temporarily decrease testosterone production at the testicular level. If you think you have low testosterone, order these testosterone tests online at an affordable price and see how your hormones are doing. References : Testosterone decrease after a mixed meal in healthy men independent of SHBG and gonadotropin levels. Andrologia. Volume 44, Issue 6 December 2012. Pages 405-410. Abrupt decrease in serum testosterone levels after an oral glucose load in men: implications for screening for hypogonadism. Clin Endocrinol (Oxf) 2013 Feb;78(2):291-6. Testosterone Test - Testing.com Testosterone as a Fasting Blood Test? - Grand Rounds in Urology Testosterone blood test – how to prepare for your blood test | healthdirect Is a fasting testosterone level really necessary for the determination of androgen status in men? - PubMed -
Testosterone production, action, and clinical manifestations
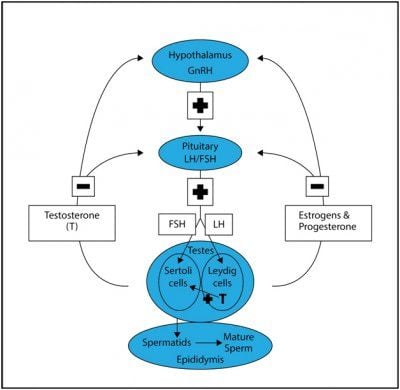
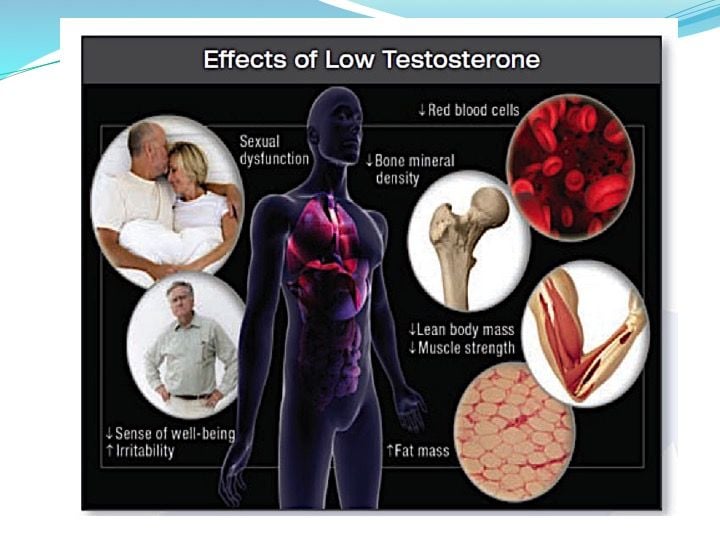
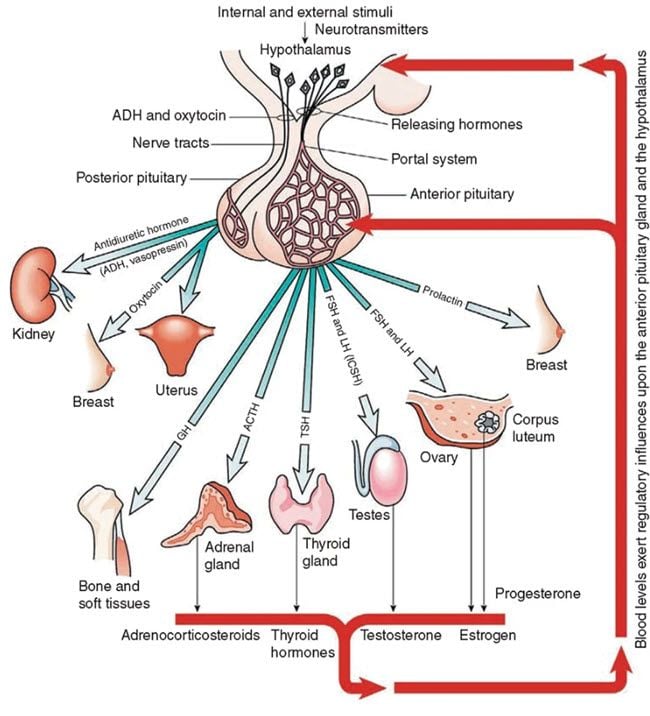
Categories: Testosterone TestsThe hypothalamus in the male body secretes GnRH pulsatilely to stimulate the release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) from the pituitary gland. LH gets to the testes through the bloodstream and binds to an LH receptor. This starts a chain of biochemical reactions that change LDL cholesterol into testosterone. The bloodstream carries the secreted testosterone from the testes to target tissues, where it produces its biological effects. Testosterone Production, Action, and Clinical Manifestations of Testosterone Deficiency in the Male Body Testosterone Production in the Male Body The pituitary gland releases follicle-stimulating hormone (FSH) and luteinizing hormone (LH) in response to the hypothalamus' pulsatile secretion of GnRH. LH gets to the testes through the bloodstream and binds to an LH receptor. This starts a chain of biochemical reactions that turn LDL cholesterol into testosterone. The bloodstream carries the secreted testosterone from the testes to target tissues, where it produces its biological effects. Hypogonadism: Testosterone Deficiency Hypogonadism is the inability of the testes to produce physiological levels of testosterone. Primary hypogonadism refers to hypogonadism resulting from abnormalities in the testes, while secondary hypogonadism refers to a defect in the hypothalamic-pituitary axis. Dual or mixed forms can also occur. If an insufficient amount of testosterone reaches the target tissues, manifestations of testosterone deficiency may appear in the liver, muscle, and adipose tissue. Mechanism of Testosterone Action Effects on Liver and Muscle Testosterone binds directly to the androgen receptor in the liver. In the liver, testosterone enhances protein synthesis. While in muscle, testosterone enhances muscle mass. Given its role in muscle, men with reduced levels of testosterone may complain of muscle weakness, lethargy, or decreased energy. Conversion to Estradiol: Effects on Brain and Bone In other tissues, testosterone must first undergo conversion before becoming biologically active. Estradiol binds to the estrogen receptor following the aromatization of testosterone in the brain and bone. Testosterone enhances bone development by promoting bone accretion. Men with reduced testosterone levels may develop osteoporosis. Testosterone acts in the brain to stabilize mood, enhance libido, and may even have a positive effect on cognition. As a result, men with testosterone deficiency can experience mood changes, a lack of motivation, and reduced libido. Conversion to Dihydrotestosterone: Effects on Skin, Hair, and Sexual Organs 5-alpha-reductase changes testosterone into dihydrotestosterone (DHT) so that it can bind to androgen receptors on hair, skin, and the prostate. Testosterone supports the growth of facial, body, axillary, and pubic hair in the adult. However, in some genetically susceptible men, testosterone may also inhibit hair growth in some areas of the scalp, leading to baldness. In the sexual organs, testosterone contributes to penile growth, spermatogenesis, and prostate growth and function. Profound hypogonadism interferes with the vascular function of the penis (corpora) and may lead to erectile dysfunction and a decrease in orgasm quality. Other Effects of Testosterone Other effects of testosterone include promotion of erythropoiesis and regulation of immune function. Clinical Manifestations of Testosterone Deficiency Men with testosterone deficiency may experience: Muscle weakness, lethargy, or decreased energy Mood changes, lack of motivation, and reduced libido Osteoporosis Erectile dysfunction and decreased orgasm quality Anemia due to decreased erythropoiesis Altered immune function Summary In summary, testosterone production plays a key role in many body tissues, and testosterone deficiency can result in a myriad of clinical manifestations. Buy a cheap testosterone test online -
Best Testosterone Book : Beyond Testosterone
Categories: Testosterone Tests , HCG Use in Men , Testosterone Side Effect Management , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , Testosterone TRT Forums , Erectile Dysfunction Lab Tests , Testosterone BookThe Best Illustrated Testosterone Book Now Available on Amazon Nelson Vergel, a well-known author of men’s health and hormone books, has published his fourth testosterone book, Beyond Testosterone. Nelson Vergel holds a chemical engineering degree and an MBA. After an HIV diagnosis over 33 years ago, he explored therapies to reverse wasting syndrome to save his life and those of his peers, leading him to co-author “Built to Survive: The Clinical Use of Anabolic Steroids for HIV+ Men and Women”,” a book that became the leading wasting treatment guide in the HIV field. He has been a member of several NIH and pharmaceutical advisory groups and FDA review panels. Nelson also founded the Body Positive Wellness Clinic and Program for Wellness Restoration in Houston, providing health education and services to HIV+ people. To expand help to the general population, he wrote “Testosterone: A Man’s Guide” and created ExcelMale.com and DiscountedLabs.com to provide men’s health education and access to affordable blood testing. His latest project aims to improve access to testosterone and hormone replacement treatments around the world by providing the largest physician directory in the world. About the Book: Beyond Testosterone This 427-page illustrated book covers all aspects of testosterone replacement therapy, including the basics of testosterone, testosterone in women, and how to increase testosterone levels naturally. It also covers the diagnosis of low testosterone and the different treatment options available by prescription in the United States and around the world. Moreover, "Beyond Testosterone" goes in-depth on the benefits of testosterone replacement therapy, side-effect management, and the effects of testosterone on the prostate and cardiovascular system. The book also reviews the uses of human chorionic gonadotropin (HCG) and discusses whether estradiol is an enemy or a friend of men. It covers the use of anastrozole and how to prevent and treat gynecomastia, acne, hair loss, water retention, high blood pressure, erectile dysfunction, and low libido. It also explores the clinical use of FDA-approved anabolic steroids for different conditions, like wasting and other diseases. Furthermore, "Beyond Testosterone" provides information on fertility and HPTA recovery after anabolic steroid use or after stopping testosterone treatment. It also covers growth hormone-releasing hormones, DHEA supplementation, thyroid dysfunction diagnosis and treatment, and maintaining good mental health. Additionally, it provides tips on nutrition for muscle gain and fat loss, exercise, and how to monitor TRT lab tests. Lastly, the book includes a section on slack testosterone in Spanish, interviews with different experts, and resources. This book is an excellent resource for men who are considering testosterone replacement therapy or are already on TRT. It is a comprehensive guide that provides information on all aspects of TRT, from diagnosis to treatment to recovery. With "Beyond Testosterone," men can have a better understanding of their options and make informed decisions about their health. Beyond Testosterone: Book Contents Introduction How to Use This Book Testosterone 101 Testosterone in Women How to Increase Testosterone Naturally Benefits of Testosterone Replacement Diagnosis of Hypogonadism (Low Testosterone) Testosterone Treatment Options Testosterone Side Effect Management Testosterone and the Prostate Testosterone and the Cardiovascular System Human Chorionic Gonadotropin (HCG) Estradiol: The Other Male Hormone Gynecomastia: Not a Simple Diagnosis Dihydrotestosterone: Should We Be Concerned About This Testosterone Metabolite? TRT-Related Acne and Hair Loss TRT-Related Water Retention and High Blood Pressure Erectile Dysfunction/Low Libido Clinical Use of FDA-Approved Anabolic Steroids Fertility and HPTA Recovery Growth Hormone-Releasing Products Thyroid Dysfunction: Diagnosis and Management Mental Health Nutritional Considerations Exercise Considerations Nelson's Tips for TRT Patients How to Monitor TRT Lab Tests La Testosterona: Información en Español Expert Interviews TRT Resources "Beyond Testosterone" is more than a medical guide; it's a tribute to the collective wisdom of the ExcelMale.com community, capturing the essence of community-driven health discussion. Each topic is enhanced with QR codes for updated information and practical tips, making it a dynamic tool for anyone seeking to understand the broader implications of testosterone in health. This book is indispensable for patients exploring testosterone therapy and clinicians aiming to enhance their therapeutic practices. It promises to empower readers with knowledge and inspire them to take charge of their health. Click here to buy: Beyond Testosterone by Nelson Vergel Click here to buy: US: Buy Now Canada: Buy Now UK: Buy Now Australia: Buy Now Spain: Buy Now Germany: Buy Now ALSO AVAILABLE ON THESE DEVICES FIRE TABLETS Fire HD 8 (8th Generation) Fire 7 (9th Generation) Fire HD 10 (9th Generation) Fire HD 8 (10th Generation) Fire HD 10 (11th Generation) Fire HD 10 Plus Fire 7 (12th Generation) Fire HD 8 (12th Generation) Fire HD 8 Plus FREE KINDLE READING APPS Kindle for Android Phones Kindle for Android Tablets Kindle for iPhone Kindle for iPad Kindle for Mac Kindle for PC Kindle for Web -
Key Pituitary And Thyroid Hormone Tests Before Starting Testosterone
Categories: Testosterone Tests , Thyroid Lab Tests , TSH Thyroid Test , Free T3 Thyroid Test , Free T4 Thyroid Test , Reverse T3 Thyroid Test , Testosterone Side Effect Management , TRT Side Effects , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , TRT Testing , TRT Monitoring , Testosterone Replacement Monitoring Tests , Thyroid Tests , LH Lab Test , FSH Fertility Test , Prolactin Lab TestTable of Contents Symptoms Of Hypogonadism (Low Testosterone) And How To Diagnose Primary and secondary hypogonadism (Low Testosterone) The pituitary gland and problems associated with it Exploring Hyperprolactinemia (High Prolactin) and Its Implications in Low Testosterone Throwing a spotlight on the pituitary and its function Pituitary imaging in the diagnosis of low testosterone Learning about thyroid and its role in low testosterone Conclusions Testosterone replacement therapy is available in many forms and can be beneficial for men who have low testosterone levels. When the body doesn't produce enough testosterone (a condition also known as hypogonadism), men can experience different symptoms such as low sex drive, fatigue, bad mood, and irritability. The body might not produce enough testosterone because of different factors. For example, the pituitary and thyroid glands play an important role in the production of testosterone and if they are not healthy, young men might experience low testosterone levels. It is important to note here that the production of testosterone decreases as men age and this is normal to be so. However, approximately 0.1% of men aged 40-49 years and about 3-5% of men aged 60-79 develop androgen deficiency which can negatively influence their lifestyle. Those who have type 2 diabetes and are obese are at a higher risk of having low blood testosterone. Before taking advantage of testosterone replacement therapy, it is important to assess the health of other organs in the body which are directly related to the production of testosterone such as the pituitary and thyroid. The pituitary gland is a very small organ situated at the base of the skull, weighing just 0.018 oz. It is responsible for releasing the growth hormone as well with the production of testosterone. If a patient is suspected of having low testosterone levels, doctors usually recommend analyzing and treating the pituitary gland as well, before opting for testosterone replacement (TRT) therapy. Similarly, the thyroid is an endocrine gland situated in the neck. It is responsible for the production of numerous hormones which help the body's metabolic processes. It also plays a vital role in the production of testosterone. Symptoms Of Hypogonadism (Low Testosterone) And How To Diagnose This type of medical condition can have various symptoms and as mentioned earlier, people who are obese or have type 2 diabetes are more likely to develop hypogonadism. Other risk factors include chronic depression, cancer, a medicine which interferes with testosterone production, chronic illness, and others. People who abuse opiates and glucocorticoids are also at a higher risk of developing hypogonadism over time. Proper testosterone production is strictly correlated with a healthy lifestyle, which involves working out regularly and eating a balanced diet. Smoking and cardiovascular diseases can also put someone at risk of developing low blood testosterone. By improving the testosterone level through replacement therapy or by treating any existing pituitary or thyroid issue, the overall quality of life can be drastically increased. For example, men who have tried testosterone replacement therapy report better sexual satisfaction, better mood, more energy and a general sense of wellbeing. In very rare cases, the testosterone level can be low because of other factors, such as extremely hard physical training. Professional athletes, especially those who compete in combat sports, might have low testosterone levels as a result of fatigue, improper nutrition, lack of rest, etc. it is important to take a look at a patient's physical condition and training regime to accurately diagnose androgen deficiency. A professional can use special tests to diagnose hypogonadism. It is important to let an experienced healthcare provider assess the testosterone levels to avoid confusion and medical complications. Proper laboratory diagnosis is done early in the morning when testosterone levels are at their peak. For accurate screening, The Endocrine Society recommends two morning (8:00-10:00 a.m.) specimens obtained on different days. Testosterone production follows something called a diurnal rhythm, meaning that the production is higher in the morning and lower at the end of the day. Working night shifts or having poor quality sleep can drastically influence the result of the analysis, so patients should take this into consideration. Similarly, having an acute illness can also render false testosterone diagnosis. It is necessary to perform 2 or more testosterone evaluations to determine if a patient is suffering from hypogonadism or not, since approximately 33% of men have a positive result after one measurement. Evaluating testosterone levels is highly recommended for certain patients, regardless if they experience the hypogonadism symptoms or not. For example, patients with HIV or those who have type 2 diabetes mellitus, osteoporosis or chronic pulmonary disease are also at a higher risk of having low serum testosterone. Once the testosterone levels have been measured and it has been confirmed that the patient might benefit from testosterone replacement therapy, additional endocrinology tests should be performed to determine the nature of the hypogonadism – primary or secondary. Treating hypogonadism accurately is paramount, especially if the patient has certain fertility goals. Primary and secondary hypogonadism (Low Testosterone) As mentioned earlier, a low testosterone level in the bloodstream might result from 2 factors. The Leydig cells located in the testes are responsible for producing the majority of testosterone in men. This process takes place using the luteinizing hormone (LH) from the pituitary gland. The LH is also strictly linked to the GnRH which is produced by the hypothalamus. The GnRH is released in a pulsatile manner and a disruption in this process can lead to low testosterone levels over time. To sum it up, men can suffer from primary hypogonadism (the testosterone is not produced in the testes), from secondary hypogonadism (the production of LH or GnRH is disrupted in the pituitary or hypothalamus) or both. If a patient has primary hypogonadism, the LH and FSH levels will be elevated as these hormones are produced by the pituitary and hypothalamus but not properly converted into testosterone. Most specialists recommend karyotype analysis for further investigation. The causes of primary hypogonadism can be multiple and they include HIV, toxins gathered in the body, acquired anorchia, orchitis, and more. On the other hand, if the LH and FSH levels are low, then additional investigations must be done to determine the nature of the secondary hypogonadism. It basically means that the testes are perfectly capable of making testosterone, but they don't have the primary resource (LH) to do so. The pituitary gland and problems associated with it Secondary hypogonadism is a more complicated medical issue and it involves looking at the characteristics of the pituitary gland. There are numerous factors which might cause secondary hypogonadism such as certain types of tumors, untreated sleep apnea, infiltrative diseases, use of certain drugs such as marijuana, opiates, and heroin, etc. Hyperprolactinemia can be a contributing factor in about 5% of secondary hypogonadism. This means that a prolactin adenoma can put pressure on the pituitary gland and cause damage. There are also different types of medications which can affect prolactin secretion, such as metoclopramide and others. In some cases, secondary hypogonadism can be caused by GnRH deficiency which happens as a result of damage to the hypothalamus. This part of the brain can become injured as a result of toxins accumulation, trauma, taking certain types of medication, as well as systemic disease. If a patient is suspected of having secondary hypogonadism, he will receive a full pituitary workup to determine prolactin levels (which requires overnight fasting for 8-10 hours) and to see if its secretion is disrupted or not. It is paramount to differentiate between secondary hypogonadism originating in the pituitary and the one originating in the hypothalamus. Men who have fertility goals and want to have children in the near future need a different type of treatment than those who don't have any fertility goals. There are rare instances when men suffer from a combination of primary and secondary hypogonadism. This might happen as a result of alcohol abuse, sickle cell disease, and more. There are several treatment options available in this case such as spermatogenesis and others. Exploring Hyperprolactinemia (High Prolactin) and Its Implications in Low Testosterone It has been discovered that men who suffer from hyperprolactinemia experience a wide variety of symptoms, such as decreased sperm mobility and low libido. These can lead to a low-quality sex life and fertility problems. Even in the presence of relatively normal testosterone levels, hyperprolactinemia can have a significant negative impact on sexual health, leading to erectile dysfunction in worst cases. By normalizing prolactin levels, scientists have discovered that testosterone levels improve and the overall quality of life is enhanced as well. Correct prolactin levels are directly associated with a healthy testosterone metabolism. Therefore, patients who have low serum testosterone should seek treatment for improving prolactin levels first before opting for testosterone replacement therapy. Once it has been discovered that the body responds well to hyperprolactinemia treatment, it might not be necessary to take advantage of testosterone replacement therapy. Throwing a spotlight on the pituitary and its function The pituitary gland plays a vital role in the production of testosterone and it should be properly assessed to determine if there are any additional hormonal imbalances present in the body. For example, for men with a testosterone level lower than 150 ng/dL, an evaluation of the anterior pituitary axes is highly recommended. This evaluation can discover other medical conditions, such as hypopituitarism, which might affect proper testosterone production. Testing the pituitary gland should be done early in the morning before 9 am with overnight fasting (8-10 hours). This is done by drawing blood to measure cortisol levels as well as ACTH. If the patient works night shifts, which might compromise the accuracy of the test, an ACTH stimulant is administered intramuscularly. This test can give insights into the hormonal balance of the patient. For example, if it is suspected that the patient has Cushing syndrome, the doctor might recommend a 1 mg dexamethasone suppression test. If acromegaly is suspected (growth hormone deficiency), then other tests are necessary to determine the exact levels of growth hormone. Such tests are required to determine the full biochemical makeup of the patient in relation to the pituitary gland and hypogonadism. If the results are positive for one or more of those tests, the patient will be redirected to endocrinology for additional measurements. Pituitary imaging in the diagnosis of low testosterone Magnetic resonance imaging (MRI) might be used to discover further details about the pituitary gland and this decision is based on multiple tests of the hormone levels. Pituitary imaging is done only when proper clinical management is required and it can be used to discover incidentalomas, which can be 6 mm in diameter or less. These are small bodies that might grow on the pituitary gland and put pressure on it which in turn disrupts the regular flow of hormones required for healthy testosterone production. These incidentalomas are usually found in approximately 20% of autopsies and can also be encountered in up to 10% of the population who is referred to pituitary imaging. The MRI testing of the pituitary should be done on men who have severe secondary hypogonadism (testosterone levels are below 150 ng/dL, persistent hyperprolactinemia, and others). Pituitary imaging isn't necessary for cases of primary hypogonadism and it is only performed when absolutely necessary. Learning about thyroid and its role in low testosterone The thyroid is very important when it comes to testosterone production. In general terms, hypothyroidism has been associated with a decrease in total testosterone levels, while hyperthyroidism might lead to converting too much testosterone into estradiol, which results in impaired sexual function, gynecomastia (enlarged man's breasts), and other medical conditions. In some cases, hypothyroidism can lead to hyperprolactinemia, but such occurrences are rare. When this happens, improving the thyroid function through certain treatments or medication can stabilize prolactin levels and this, in turn, will normalize testosterone production. Hypothyroidism is also frequently associated with erectile dysfunction. Similarly, hyperthyroidism can also be problematic, as it has been associated with ejaculatory dysfunction, as shown in a study done on over 750 men. More than 50 percent of those who had hyperthyroidism also showed symptoms of reduced sperm mobility and ejaculatory problems. However, when these men received treatment for hyperthyroidism, their fertility and testosterone production improved significantly, which means that testosterone replacement therapy isn't necessarily the go-to treatment for all men suffering from androgen deficiency. Conclusions As presented in this article, the human body is very complex, and there might be multiple causes for a low serum testosterone level in the bloodstream on males of all ages. It is important to determine whether the hypogonadism is primary or secondary, as well as perform numerous tests and hormone evaluations to determine the nature of the hypogonadism and to prescribe the correct treatment. In case the pituitary gland is the culprit, MRI tests might be required, though such instances are rare. Certain types of treatments are also recommended if the patient has fertility goals. If none of the other medications and treatments for hypogonadism are accurate, then testosterone replacement therapy might be considered for certain patients. By the way, monitoring serum testosterone, LH, FSH and prolactin is very easy these days thanks to tests that can be bought online at discounted prices. Visit www.discountedlabs.com for more details. -
Estradiol and DHT Levels on TRT: How to Predict
Categories: Estradiol Test , Testosterone Tests , Testosterone Side Effect Management , TRT Side Effects , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , TRT Testing , TRT Monitoring , Testosterone Replacement Monitoring TestsTestosterone Replacement Therapy (TRT) is a common treatment for men with low testosterone levels. While TRT can have numerous benefits, such as increased energy, libido, and muscle mass, it is important to monitor other hormone levels, specifically estradiol and dihydrotestosterone (DHT). While DHT is a metabolite of testosterone, estrogen is a form of estrogen that results from the aromatization of testosterone. Understanding the optimal levels of these hormones on TRT is crucial for achieving the desired effects while minimizing potential side effects. In this article, we will discuss a study conducted on young and older men using different doses of testosterone and its implications for predicting estradiol and DHT levels on TRT. Table of Contents The Study: Testosterone Injections and Estradiol/DHT Levels Results and Findings Estradiol Levels DHT Levels Predictive Model Interpreting the Findings Conclusion The Study: Testosterone Injections and Estradiol/DHT Levels The study in question was conducted by researchers at Boston University School of Medicine and published in the Journal of Clinical Endocrinology & Metabolism in 2010. The aim of the study was to investigate the effects of different doses of testosterone injections on estradiol and DHT levels in young and older men. The participants included 51 young men aged 19 to 35 and 50 older men aged 59 to 75. To conduct the study, the participants were administered a blocker to suppress their natural testosterone production. They were then given weekly injections of different doses of testosterone for a duration of five months. The researchers measured the participants' estradiol and DHT levels throughout the study to assess the impact of testosterone doses on these hormones. Results and Findings The study revealed several interesting findings regarding estradiol and DHT levels in men on TRT. Here are some key points: Estradiol Levels The study found that estradiol levels increased with increasing doses of testosterone in both young and older men. However, the increase in estradiol was more significant in older men compared to younger men. This suggests that older men may have a higher propensity for aromatization, which is the conversion of testosterone into estradiol. It is important to note that the estradiol levels observed in the study were higher than the reference ranges provided by some laboratories, which are primarily derived from men not on TRT. DHT Levels DHT levels also increased with higher testosterone doses, but the difference between young and older men was not as pronounced as with estradiol. DHT is derived from testosterone through the action of the enzyme 5-alpha reductase. While DHT is often associated with androgenic side effects, such as male pattern baldness and prostate enlargement, its role in TRT is still not fully understood. Predictive Model To help predict estradiol and DHT levels based on testosterone dose, the researchers developed a mathematical model using the data from the study. The model provides equations to estimate estradiol and DHT levels based on total testosterone levels. These equations can be helpful for clinicians and individuals on TRT to better understand and predict their hormone levels. Interpreting the Findings The findings from this study have important implications for individuals on TRT. It is essential to recognize that estradiol levels on TRT may be higher than the reference ranges established for men not on TRT. This is because the reference ranges are typically derived from individuals with lower testosterone levels. It is crucial to consider the individual's specific situation and response to TRT when interpreting estradiol levels. Additionally, the study emphasizes the need for regular monitoring of hormone levels to ensure they are within a safe and optimal range. By measuring estradiol and DHT levels, healthcare providers can make informed decisions regarding dosage adjustments and potential interventions to manage any adverse effects. It is important to remember that individual responses to TRT can vary, and what may be considered an optimal hormone level for one person may not be the same for another. Factors such as age, overall health, and personal preferences should be taken into account when evaluating hormone levels and making treatment decisions. Conclusion Understanding the impact of testosterone replacement therapy on hormone levels, particularly estradiol and DHT, is crucial for optimizing the benefits and minimizing the risks associated with TRT. The study discussed in this article provides valuable insights into the effects of different testosterone doses on estradiol and DHT levels in men. It is essential for individuals on TRT to work closely with healthcare professionals who can monitor hormone levels regularly and guide them in making informed decisions about their treatment. The predictive model developed in the study can serve as a helpful tool in estimating estradiol and DHT levels based on testosterone dose, but individual variations should always be taken into account. By monitoring hormone levels and adjusting treatment accordingly, individuals on TRT can achieve the desired effects while minimizing potential side effects. Regular communication with healthcare providers is key to ensuring the effectiveness and safety of testosterone replacement therapy. Disclaimer: The information in this article is based on the findings of a specific study and should not replace personalized medical advice. Individuals on TRT should consult with qualified healthcare professionals to address their specific needs and concerns. -
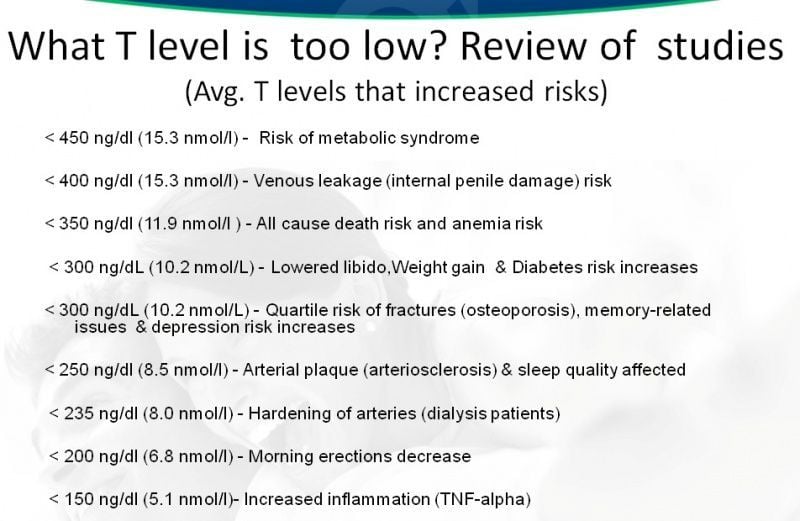
The Underestimated Risks of Low Testosterone Levels: A Comprehensive Guide
Categories: Testosterone Tests , Free T4 Thyroid Test , Testosterone Side Effect Management , TRT Side Effects , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , TRT Testing , TRT Monitoring , TRT Guidelines , Testosterone Replacement Monitoring Tests , Men's Health Lab TestsTestosterone is more than just a sex hormone. It plays a crucial role in a range of physiological processes, including the development of muscle mass, bone density, and even the modulation of blood sugar levels. While high levels of testosterone can have their own set of complications, this article focuses on the often-underestimated risks associated with low testosterone levels. What is Low Testosterone? Low testosterone is a condition where the body does not produce sufficient amounts of the hormone. The threshold for low testosterone varies, but it is generally considered to be below 300 ng/dL (nanograms per deciliter) for adult men. The condition can lead to various health issues, ranging from metabolic syndrome to increased risk of death from all causes. Understanding the Causes of Low Testosterone: Testosterone, the primary male sex hormone, plays a crucial role in maintaining a range of bodily functions, from muscle mass and fat distribution to bone density and red blood cell production. While it's common for testosterone levels to decline as men age, significantly low levels can lead to a host of health issues. But what causes low testosterone levels? The reasons are many and can range from genetic conditions to lifestyle choices. Let's break it down. Secondary Causes: Hypothalamic-Pituitary Dysfunction Idiopathic GnRH Deficiency, Kallman Syndrome, and More Sometimes, low testosterone can be due to issues with the pituitary gland or the hypothalamus, parts of the brain that signal the testicles to produce testosterone. Conditions such as Idiopathic GnRH deficiency and Kallman syndrome can disrupt these signals. These conditions are examples of hypogonadotropic hypogonadism (Bhasin et al., 2010). Inflammatory Causes Inflammation of the pituitary gland can also result in low testosterone. This inflammation can be due to a variety of factors, including autoimmune reactions and certain illnesses (Dandona & Rosenberg, 2010). Trauma and Tumors Blunt head trauma or postsurgical complications can affect the pituitary gland, leading to low testosterone. Tumors like pituitary adenomas or craniopharyngiomas can have similar effects (Wu et al., 2010). Vascular Insult Issues with the blood vessels that supply the pituitary, such as pituitary infarct/apoplexy or carotid aneurysm, can also be a culprit. Drug-Induced Causes Certain medications like anabolic steroids, opioids, and drugs that induce hyperprolactinemia can contribute to low testosterone. Always consult your doctor if you are on medication and experiencing symptoms of low testosterone (Bhasin et al., 2010). Systematic Illness and Autoimmune Causes Chronic illnesses such as anorexia nervosa, chronic renal failure, and liver failure can result in low testosterone. Autoimmune conditions that attack the pituitary gland (autoimmune hypophysis) can also be a factor (Dandona & Rosenberg, 2010). Primary Cause: Testicular Dysfunction Chromosomal and Genetic Factors Issues right at the level of the testicles can also be causes. Conditions like Klinefelter's syndrome, XX male gonadal dysgenesis, and defects in androgen biosynthesis are all chromosomal abnormalities that can lead to low testosterone (Wu et al., 2010). Infections and Surgeries Orchitis (inflammation of the testicles due to infections like mumps or HIV) and orchiectomy (surgical removal of the testicle) can directly affect testosterone production. Other Factors Chronic infections like tuberculosis, irradiation, testicular torsion, and certain medications can also be responsible. Lifestyle and Other Factors Factors like obesity, aging, malnutrition, and exposure to toxins such as heavy metals and alcohol can also influence testosterone levels (Dandona & Rosenberg, 2010). Low testosterone can result from a variety of causes, ranging from medical conditions and medications to lifestyle choices. If you're experiencing symptoms, it's crucial to consult a healthcare provider for a comprehensive diagnosis and treatment plan. Risks Associated with Different Levels of Low Testosterone < 450 ng/dl (15.3 nmol/l) - Risk of Metabolic Syndrome Metabolic syndrome is a cluster of conditions that include high blood pressure, elevated blood sugar levels, excess body fat, and abnormal cholesterol levels. Testosterone plays a significant role in regulating these physiological functions. Research by Dhindsa et al. has highlighted the increased risk of metabolic syndrome in men with testosterone levels below 450 ng/dl1. < 400 ng/dl (15.3 nmol/l) - Venous Leakage (Internal Penile Damage) Risk Venous leakage is a condition that can result in erectile dysfunction due to internal penile damage. According to a study by Yassin and Saad, men with testosterone levels below 400 ng/dl are at a higher risk of developing this condition2. < 350 ng/dl (11.9 nmol/l) – All-Cause Death Risk and Anemia Risk Khaw et al. conducted a study that showed men with testosterone levels below 350 ng/dl had an increased risk of death from all causes, as well as a higher risk of developing anemia3. < 300 ng/dL (10.2 nmol/L) - Lowered Libido, Weight Gain & Diabetes Risk Increased A low level of testosterone can also have a detrimental effect on sexual health, including a decrease in libido. Furthermore, it is associated with weight gain and an increased risk of developing diabetes. Traish et al. discussed these risks in their research4. < 300 ng/dL (10.2 nmol/L) - Quartile Risk of Fractures (Osteoporosis), Memory-Related Issues & Depression Risk Increases Testosterone is crucial for bone density. Low levels can increase the risk of fractures, memory-related issues, and even depression. A study by Orwoll et al. emphasized these risks5. < 250 ng/dl (8.5 nmol/l) - Arterial Plaque (Arteriosclerosis) & Sleep Quality Affected Vlachopoulos et al. found that men with testosterone levels below 250 ng/dl had a higher risk of developing arterial plaque, which can lead to arteriosclerosis. Additionally, these men experienced a reduction in sleep quality6. < 235 ng/dl (8.0 nmol/l) - Hardening of Arteries (Dialysis Patients) Carrero et al. identified that low testosterone levels can increase the mortality risk among male dialysis patients by promoting the hardening of arteries7. < 200 ng/dl (6.8 nmol/l) - Morning Erections Decrease A study by O'Connor et al. showed that men with testosterone levels below 200 ng/dl experienced a decrease in morning erections, which is often a sign of erectile dysfunction8. < 150 ng/dl (5.1 nmol/l) - Increased Inflammation (TNF-alpha) Malkin et al. found that extremely low levels of testosterone, under 150 ng/dl, were associated with increased inflammation markers like TNF-alpha9. Conclusion Low levels of testosterone are linked to a wide range of health issues. While testosterone replacement therapy is often recommended for men with low levels, understanding the risks associated with varying degrees of low testosterone is crucial for effective treatment and prevention. Always consult your healthcare provider for diagnosis and treatment. Buy a Low Cost Total and Free Testosterone Test on DiscountedLabs.com: Testosterone test near me. Low Testosterone: What Do Different Medical Guideline Groups Say? Understanding the guidelines for diagnosing and treating low testosterone is crucial for both healthcare providers and patients. Different medical organizations have released various guidelines over the years, making it essential to know how each defines low testosterone levels. This article aims to shed light on what various medical guideline groups have to say about low testosterone, focusing on cutoff values and expert opinions. Expert Opinion Before delving into specific guidelines, it's worth noting that expert opinion often plays a significant role in forming these guidelines. Medical professionals and researchers contribute to these guidelines based on clinical experience, existing studies, and ongoing research. Therefore, guidelines are not static but evolve over time, reflecting the current state of medical knowledge. Year of Release and Update Knowing when a particular guideline was released or updated is important as it indicates the currency and relevancy of the information. Here is a brief timeline: ISSAM: 2005 Endocrine Society: 2006 ISSM: 2008 AUA: 2015 ICSM: 2015, updated in 2018 Cutoff Values of Testosterone for Laboratory Diagnosis One of the most critical aspects of diagnosing low testosterone is determining the cutoff values. Various organizations have different parameters. Here's a summary: Guideline Group Cutoff Values for Total T (TT) Cutoff Values for Free T Year ISSAM TT < 231 ng/dL (8 nmol/L) N/A 2005 Endocrine Society TT: 231-346 ng/dL (8-12 nmol/L) Free T < 52 pg/mL 2006 ISSM TT < 230 ng/dL (8 nmol/L) Free T < 52 pg/mL 2008 AUA TT: 230-350 ng/dL (8-12 nmol/L) Free T < 65 pg/mL 2015 ICSM TT < 300 ng/dL Free T < 5 ng/dL 2018 Definitions and Abbreviations: ISSAM: International Society for the Study of the Aging Male ISSM: International Society for Sexual Medicine ICSM: International Consultation for Sexual Medicine AUA: American Urological Association TT: Total Testosterone Free T: Free Testosterone SHBG: Sex Hormone-Binding Globulin Understanding the various guidelines for diagnosing low testosterone is crucial for appropriate treatment. It's evident that different medical organizations have varying cutoff values, and these may be subject to change as more research becomes available. Always consult your healthcare provider for the most current and personalized advice. By keeping updated on these guidelines, both physicians and patients can make more informed decisions regarding the diagnosis and treatment of low testosterone. Sources: International Society for the Study of the Aging Male (ISSAM), Guidelines, 2005. Endocrine Society, Clinical Guidelines, 2006. International Society for Sexual Medicine (ISSM), Guidelines, 2008. American Urological Association (AUA), Guidelines, 2015. International Consultation for Sexual Medicine (ICSM), Guidelines, 2015, updated in 2018. Footnotes Dhindsa, S., Miller, M. G., McWhirter, C. L., Mager, D. E., Ghanim, H., Chaudhuri, A., & Dandona, P. (2010). Testosterone concentrations in diabetic and nondiabetic obese men. Diabetes Care, 33(6), 1186-1192. PubMed ↩ Yassin, A. A., & Saad, F. (2017). Testosterone Deficiency and Testosterone Treatment in Older Men. Gerontology, 63(2), 144–156. PubMed ↩ Khaw, K. T., Dowsett, M., Folkerd, E., Bingham, S., Wareham, N., Luben, R., ... & Day, N. (2007). Endogenous testosterone and mortality due to all causes, cardiovascular disease, and cancer in men. Circulation, 116(23), 2694-2701. PubMed ↩ Traish, A. M., Saad, F., & Guay, A. (2009). The dark side of testosterone deficiency: I. Metabolic syndrome and erectile dysfunction. Journal of Andrology, 30(1), 10-22. PubMed ↩ Orwoll, E., Lambert, L. C., Marshall, L. M., Phipps, K., Blank, J., Barrett-Connor, E., ... & Cummings, S. (2006). Testosterone and estradiol among older men. The Journal of Clinical Endocrinology & Metabolism, 91(4), 1336-1344. PubMed ↩ Vlachopoulos, C., Ioakeimidis, N., Miner, M., & Aggelis, A. (2014). Testosterone deficiency: a determinant of aortic stiffness in men. Atherosclerosis, 233(1), 278-283. PubMed ↩ Carrero, J. J., Qureshi, A. R., Parini, P., Arver, S., Lindholm, B., Bárány, P., ... & Stenvinkel, P. (2009). Low serum testosterone increases mortality risk among male dialysis patients. Journal of the American Society of Nephrology, 20(3), 613-620. PubMed ↩ O'Connor, D. B., Lee, D. M., Corona, G., Forti, G., Tajar, A., O'Neill, T. W., ... & EMAS Study Group. (2011). The relationships between sex hormones and sexual function in middle-aged and older European men. The Journal of Clinical Endocrinology & Metabolism, 96(10), E1577-E1587. PubMed ↩ Malkin, C. J., Pugh, P. J., Jones, R. D., Kapoor, D., Channer, K. S., & Jones, T. H. (2004). The effect of testosterone replacement on endogenous inflammatory cytokines and lipid profiles in hypogonadal men. The Journal of Clinical Endocrinology & Metabolism, 89(7), 3313-3318. PubMed ↩