Page 6 - Search "estradiol"
-

Testosterone Replacement Therapy- Target Blood Test Limits
Categories: TRT Testing , TRT Monitoring , TRT Guidelines , Testosterone Replacement Monitoring TestsTestosterone replacement therapy is an important treatment option for men with low testosterone and symptomatic hypogonadism. Various formulations of exogenous (supplemental) testosterone replacement therapy exist, including oral, buccal, intramuscular, transdermal, subdermal, and nasal preparations. However, exogenous testosterone replacement therapy is a double-edged sword, posing risks to fertility due to negative feedback mechanisms on the hypothalamic-pituitary-gonadal (HPG) axis, which is the primary regulator of testosterone production and sperm production in men. Testosterone replacement therapy (TRT) is one of the most effective ways to combat low testosterone levels, but you must understand the risks associated with the treatment. As with any hormone replacement therapy, there are a few downsides to receiving regular testosterone injections. But do these risks outweigh the benefits? That’s a decision you’ll have to make for yourself! Testosterone replacement therapy- Target Blood Test Limits: To minimize TRT side effects, different medical guideline groups have created lab test value ranges and maximum acceptable targets . These values have been collected from three TRT guidelines and clinical practices around the United States: Hematocrit (percent of red blood cells in plasma) under 53 PSA (Prostatic specific antigen) under 3 (4 is max since doctors will not prescribe TRT at this number) Estradiol (sensitive) between 20-50 pg/mL. However, if you have high testosterone, estradiol will be "high" per Quest or Labcorp since 0.4% of total testosterone aromatizes to estradiol. Blood pressure under 135/85 Estimated Glomerular (eGFR) (kidney function) over 60 Liver enzymes not elevated over 20 percent of top value of reference range Total Testosterone over 450 ng/dL Free Testosterone equal or above 2 percent of total If donating blood to bring hematocrit down, ferritin should never under 30 ng/mL or micrograms/liter (this could lead to fatigue) Free T3 (if hypothyroid and on treatment) in the upper quartile of range. (depending on range it can be 3.7- 4.2 pg/mL) HDL over 40 mg/dL (higher TRT doses can lead to decreased HDL cholesterol) You can order these lab tests here: TRT Male Hormone/Wellness Follow-Up Panel PSA Lipid Panel Thyroid Panel -
How to Minimize TRT Side Effects
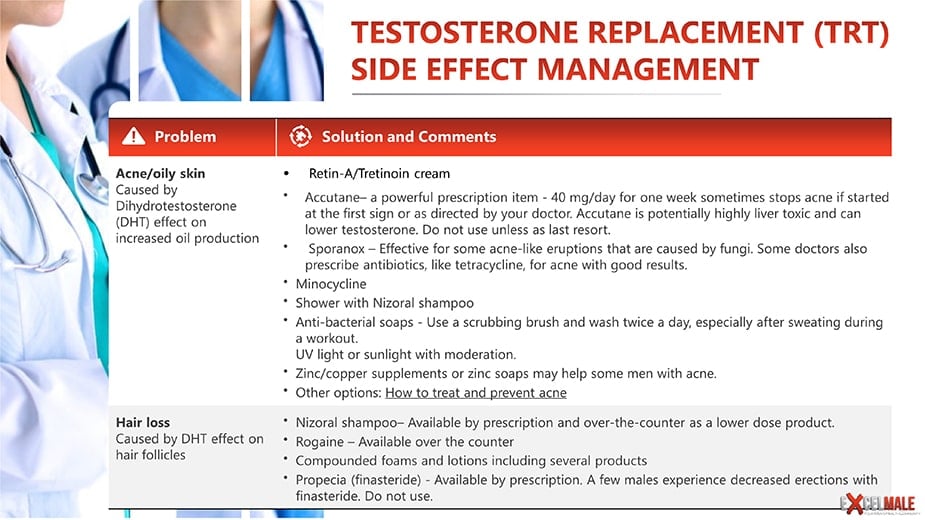
Categories: High Hematocrit , Testosterone Side Effect Management , TRT Side Effects , Estradiol Estrogen Tests for MenTRT Side Effects: How to Manage Them What are the Main Side Effects of Testosterone Replacement Therapy (TRT)? Acne/oily skin Hair loss Increased sex drive Unresolved erectile dysfunction Insomnia Sleep Apnea Testicular atrophy Enhanced assertiveness or reactivity High blood pressure/water retention Gynecomastia (male breast development) Understanding Testosterone Replacement Therapy (TRT) Testosterone replacement therapy (TRT) is a medical treatment designed to restore normal testosterone levels in men with hypogonadism, a condition where the testicles do not produce enough testosterone. This therapy aims to alleviate symptoms such as low libido, fatigue, and decreased muscle mass, which are commonly associated with low testosterone levels. TRT involves administering testosterone through various methods, including injections, gels, patches, and oral medications. By restoring testosterone levels, TRT helps improve overall quality of life for men suffering from androgen deficiency syndromes. What are the Main Side Effects of Testosterone Replacement Therapy (TRT)? Like all treatments, testosterone therapy is associated with a number of known risks, particularly for men with testosterone deficiency. These risks should be communicated to patients prior to initiation of treatment. A key item is impaired spermatogenesis (sperm production) due to suppression of gonadotropins (LH and FSH). Men considered candidates for TRT should be questioned as to their desire to induce a pregnancy. Since sperm production may be reduced to zero, exogenous T alone should be avoided until fertility is no longer a concern. Treatment with hCG injections or oral clomiphene citrate may be considered in these men, as they do not suppress spermatogenesis. There is some limited data on the use of testosterone plus hCG for improvement of sperm quality and quantity in men. Acne may occur in younger men. Edema can be occasionally observed in middle-aged or older men due to the fluid-retentive properties of testosterone. Erythrocytosis (increased red blood cell count that causes high hematocrit) is infrequently seen with topical and injectable TRT treatments but is routinely observed in men treated parenterally with short-acting injections or implanted pellets. Although there is no evidence to date that T-induced erythrocytosis is associated with adverse events, it seems reasonable to prevent the hematocrit from rising excessively. Men whose hematocrit rises above 54% (or hemoglobin greater than 18 g/dL) should be considered for dose reduction, temporary discontinuation of T therapy, blood donation, or therapeutic phlebotomy. Read this first since it is the most common testosterone side effect: High hematocrit Acne/oily skin Caused by Dihydrotestosterone (DHT) effect on increased oil production · Accutane– a powerful prescription item - 40 mg/day for one week sometimes stops acne if started at the first sign or as directed by your doctor. Accutane is potentially highly liver toxic and can lower testosterone. Do not use unless as last resort.· Sporanox—Effective for some acne-like eruptions that are caused by fungi. Some doctors also prescribe antibiotics, like tetracycline, for acne with good results.. Minocycline. Shower with Nizoral shampoo. Anti-bacterial soaps: use a scrubbing brush and wash twice a day, especially after sweating during a workout.· UV light or sunlight with moderation.. Zinc/copper supplements or zinc soaps may help some men with acne.. Other options: How to treat and prevent acne Hair loss Caused by DHT effect on hair follicles · Nizoral shampoo—Available by prescription and over-the-counter as a lower-dose product.· Rogaine—Available over the counter· Propecia - Available by prescription. A few males experience decreased erections with finasteride. Do not use. Increased sex drive · A problem? Sex drive is part of quality of life. Testosterone therapy may somewhat improve sexual function in men with low testosterone levels. This is not necessarily a bad side effect. Enjoy it. Unresolved erectile dysfunction · ED Medications: Available by prescription; enables robust erections. If you have sinus congestion or headaches/backaches, take non-drowsy allergy medication and ibuprofen. ED drugs can be combined with alpha-blockers and/or nitric oxide precursor amino acids (arginine or citrulline).· Yohimbine (Yocon) - Available by prescription; increases sex organ sensitivity. Can increase heart rate and blood pressure· Muse—Available by prescription; a pellet is inserted into the urethra to produce an erection. Unpopular· Trimix – Available by prescription from compounding pharmacies. The best and cheapest formula for injection into the penis for lasting erections.· Caverject - Available by prescription. An injection into the penis that produces an erection that can last 1 to 2 hours. Be careful with injecting too much since it can produce dangerously long erections that need to be treated in emergency rooms! Follow instructions from your urologist.· Papaverine—an older injectable medication, less expensive than Caverject.· Wellbutrin—prescription at 300 to 450 mg/day; increases dopamine.· HCG—First dose is 2,000 IU, then 250-500 IU twice or three times a week. No protocol has been proven in controlled studies yet. When Testosterone Replacement Doesn't Lead to Better Erections Insomnia Usually, this is caused by dosages that are too high. Find the least amount that gives you a good result. · Sleeping medications—e.g., Ambien, Sonata, Lunesta, Restoril· Melatonin: 1 to 3 mg before bedtime. If you wake up groggy after 6 hours, your dose should be lower.· Avoid working out too close to bedtime.· Limit caffeine, especially after 3 pm.· You may want to try a sleep formula with tryptophan, melatonin, and magnesium. Nutrients do not work as well as drugs, but they can help some people.Article: How to protect your circadian rhythm Unresolved Fatigue · Have your doctor prescribe a sleep study if you snore and wake up tired even after 7 hours of sleep. Some people may have to wear a C-PAP machine to breathe at night. Visit Home - SleepApnea.org for more information. There are also oral devices for those people who fail CPAP. Fatigue—When Testosterone Is Not Enough Testicular atrophy · HCG– One 2,000-unit injection per week for 2 weeks, followed by maintenance of 350-500 IU twice a week. Decrease testosterone dosage accordingly after starting hCG to reach levels around 500-1200 ng/dL while keeping all other lab work monitored. Watch this video on hCG and men Enhanced assertiveness or reactivity · Make sure you are getting enough sleep.. Count until 10 and be aware of your interaction with others.· Decrease caffeine.· Meditation, mindfulness, yoga; breathe from your belly for a few minutes when overreacting.· The testosterone dosage may be too high.· Ask yourself: Do I need to always be right?. Vent extra energy at the gym, sex, and sharing with your buddies at www.excelmale.com High blood pressure/water retention · Caused by sodium retention in the kidneys. Try to limit salt consumption. Caution is required due to potential water retention issues in patients with chronic kidney disease. . Blood pressure medications - Elevated blood pressure may be transient or not. Try ACE or ARBs since they seem to have fewer sexual dysfunction-related effects. · Magnesium (600 mg/day); vitamin B6 (100 to 200 mg/day); may help reduce water retention. · Water - Drink extra water every day to help flush the kidneys. . Check your estradiol to make sure it is not over 45 pg/ml. Treat if high with a low dose of anastrozole. . Make sure you are doing cardio exercise at least 3 times a week for 30 min. Sweat and lower your salt intake since TRT increases sodium retention in some men. Gynecomastia (male breast development) Caused by high estradiol in the presence of low testosterone. This is rare in men on testosterone replacement. · Arimidex inhibits estrogen production. Available by prescription. 0.25 mg per week. There is no agreement on what the highest E2 level is for men on TRT with high testosterone. Ensure that your estradiol does not go too low (under 20 pg/ml) if you use anastrozole since it is needed for bone, skin, brain, lipids, libido, good lipids and hair health.· Nolvadex (tamoxifen)– Competes with estrogen for receptors. Available by prescription, 10 to 20 mg/day. Use of Nolvadex during a steroid cycle may reduce the net anabolic effect, as it decreases the production of GH and IGF-1. High IGF-1 may be implicated in gynecomastia.. Severe cases may require removal of the breast tissue by surgery.· DHT cream- Some people have obtained great results by rubbing a 10% DHT cream on their nipples. Not available in the US but some people order it online from Germany. Read about medications/foods to avoid if you have gynecomastia.. Those who do know to respond to the above check other reasons. Find out how long it takes testosterone replacement to potentially show benefits For affordable blood tests in most cities in the U.S. : DiscountedLabs.com More information on TRT lab tests. Monitoring and Testing During TRT Regular monitoring and testing are essential during TRT to ensure safe and effective treatment. This includes: Regular blood tests to check testosterone levels, PSA, hematocrit, and liver enzymes Baseline bone density testing (DEXA) and bi-yearly bone density tests Monitoring of prostate health through PSA levels and DREs Regular check-ups with a healthcare provider to discuss any concerns or side effects These tests help in tracking the effectiveness of the therapy and in identifying any potential issues early, ensuring that the treatment remains beneficial and safe. When to Seek Care It is essential to seek medical attention immediately if any of the following occur during TRT: Symptoms of a cardiovascular event, such as chest pain or shortness of breath Severe side effects, such as acne, hair loss, or mood changes Changes in prostate health, such as increased PSA levels or abnormal DRE results Concerns about testosterone levels or overall health By understanding the benefits and risks of TRT, monitoring prostate health, and seeking care when necessary, men with hypogonadism can safely and effectively manage their condition and improve their overall quality of life. Regular communication with healthcare providers and adherence to recommended monitoring protocols are key to successful testosterone replacement therapy. References: [i] Metzger, DL, et al. Estrogen receptor blockade with tamoxifen diminishes growth hormone secretion in boys: evidence for a stimulatory role of endogenous estrogens during male adolescence. J Clin Endocrinol Metab (1994) 79(2):513-518. [ii] el-Sheikh, MM, et al. The effect of Permixon (saw palmetto) on androgen receptors. J Acta Obstet Gynecol Scand (1988) 67(5):397-399. [iii] Suzuki, K, et al. Endocrine environment of benign prostatic hyperplasia: prostate size and volume are correlated with serum estrogen concentration. Scand J Urol Nephrol (1995) 29:65-68. [iv] Gann, PH, et al. A prospective study of plasma hormone levels, nonhormonal factors, and development of benign prostatic hyperplasia. The Prostate (1995) 26:40-49. Buy your own on DiscountedLabs.com -
How to Treat Low Testosterone in Women: Treatment Options
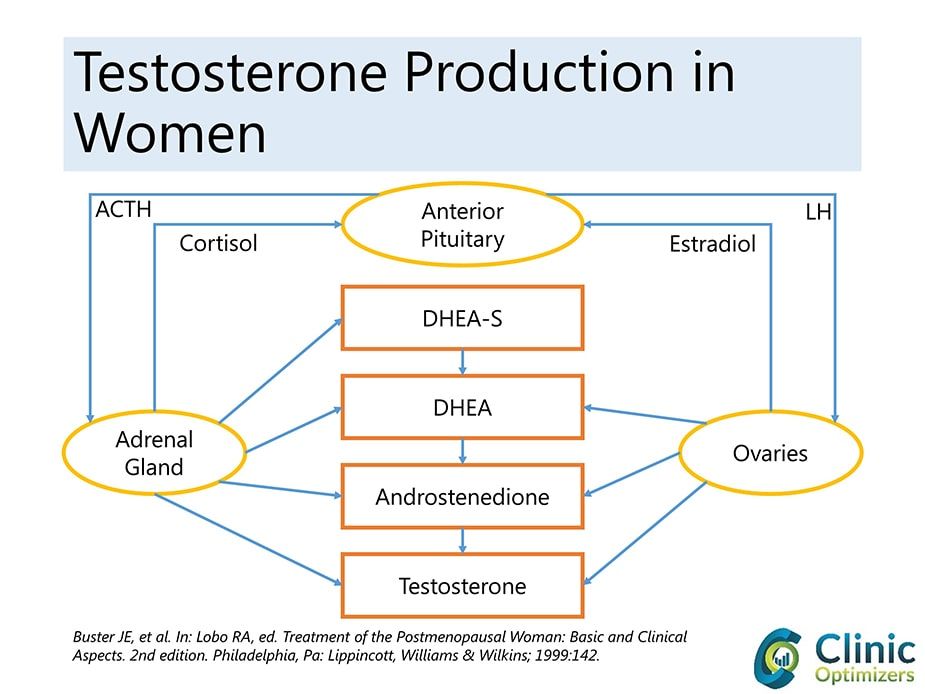
Categories: Testosterone Tests , Testosterone Blood Tests , Testosterone in Women , lab tests for women , Women's Hormone TestsTestosterone is typically thought of as a hormone for men. Still, it is also essential for women as it influences sexual functioning, mood, the development of lean muscle mass, and even memory and cognition. Women who are in their 40s have about half the level of testosterone that was present in their 20s. We see a significant decline in testosterone levels over time. Women with low or suboptimal testosterone levels can experience many symptoms, including sexual dysfunction and a decrease in sexual drive or desire, known as low sex drive (hypogonadism). They can also notice that they have increased fatigue. They're tired. Also, it's more challenging to develop lean muscle mass. It can have a significant impact even on mood, an overall sense of well-being, motivation, a feeling of confidence, and assertiveness. Also, it can affect memory and cognitive function. A low libido: As testosterone helps fuel a healthy sex drive, a decline in sexual interest or inability to achieve orgasm may be a symptom of lower testosterone levels in both sexes. A study published in the journal of the American Medical Association showed that approximately 43% of postmenopausal women suffer from some form of sexual dysfunction. Surprisingly, we don't hear a lot about this condition in women. We certainly don't hear about options for treatment, including testosterone. This condition can often go undiagnosed and undertreated. NO FDA-APPROVED TREATMENTS FOR LOW TESTOSTERONE ON WOMEN Currently, there is no FDA-approved testosterone replacement therapy for women, even though providers have been prescribing it in an off-label manner, which is when a medication is prescribed for something other than its official FDA-approved indication. Providers have been doing this for over 50 years now. Testosterone can be replaced in various forms. It can be given in a shallow-dose injection once a week. It can also be given sublingually in a troche form, which dissolves in the mouth. Also, it can be administered through a minor surgical procedure. It's known as subcutaneous pellet insertion. And then it can also be given in topical form as a cream or a gel. The most common form of replacement we see is topical gel or cream, which can be supplied by compounding pharmacies. The benefit of doing it this way is that the provider can adjust the dose based on the individual patient's needs and response to therapy. It's more than just one standard dose, and it better work for you, or there's no other option. Testosterone creams can be customized for the needs of the individual patient. When you replace any hormone in this manner at low daily doses, it is very similar to the way the body naturally produces hormones. After starting testosterone replacement therapy, women typically notice a significant improvement in all symptoms, including increased sexual functioning, desire, and drive. They can also see an increase in energy levels and an increased ability to develop lean muscle mass. Additionally, they can notice a significant improvement in mood, motivation, overall sense of well-being, and confidence. In addition, they may see improved memory and cognitive functioning. Another critical point is that when testosterone is given to a woman, a portion of it will convert to estrogen. The postmenopausal woman with low estrogen levels can see improvement in those symptoms typically associated with low estrogens, such as hot flashes, night sweats, moodiness, irritability, and vaginal dryness. So, women may experience improvements in the classic symptoms of low testosterone and the typical menopausal symptoms associated with low estrogen. Several studies support the use of hormone replacement therapy, specifically testosterone replacement therapy, in women. A Cochrane review of the literature found that over 35 trials have been performed, which included over 4500 women. They found a significant improvement in sexual functioning in women on hormone replacement therapy. Also, a more recent study published in 2014 showed that women on a transdermal or topical form of hormone replacement therapy had an improvement in memory and cognitive functioning. Several studies support the use of this vital hormone in women. POTENTIAL SIDE EFFECTS OF TESTOSTERONE IN WOMEN In terms of safety, there are potential side effects with the use of any medication. In testosterone therapy, if doses are too high, women can notice adverse effects, such as acne and an increase in hair growth, known as hirsutism. Also, with extremely high doses, they may see a deepened voice or enlargement of the labia or clitoris. That would typically be something that's dose-dependent. If a physician was a little bit aggressive with their starting dose, they might notice some side effects of testosterone treatment, such as disturbed breathing while sleeping, breast swelling or tenderness, swelling in the ankles, or too much testosterone. Doctors also watch out for high red blood cell counts, which could increase the risk of clotting. By decreasing and backing off on the dosage, those symptoms will resolve. One important fact to mention for premenopausal women who are still menstruating is that providers need to discuss the use of birth control with them because testosterone is considered category X, meaning it will cause fetal harm if a woman becomes pregnant while she's on testosterone replacement. That's just a discussion that the patient needs to have with their provider, “What is your reliable form of birth control?" before prescribing it to them. Testosterone replacement therapy is very safe for premenopausal women on birth control and postmenopausal women. It has a low risk of side effects when used at appropriate doses, and many studies support its use in this population. SEXUAL DYSFUNCTION AND LOW TESTOSTERONE IN WOMEN We are all aware that if we watch TV for more than an hour each day, we will constantly see advertisements for medications to treat erectile dysfunction in men. But we hardly hear anything about sexual dysfunction in women. There are many reasons why women’s sexual desire and other hormone-related quality-of-life issues are so misunderstood, underdiagnosed, and undertreated. Sexual dysfunction in pre and post-menopausal women has been a very controversial topic that has been poorly researched, even though a February 1999 study published in the Journal of the American Medical Association, titled “Sexual Dysfunction in the United States: Prevalence and Predictors,” found that approximately 43% of postmenopausal women suffer from some form of female sexual dysfunction. It wasn’t until June 2011 that an FDA advisory committee to the division of Reproductive and Urologic Drug Products stated that HSDD (Hypoactive Sexual Desire Syndrome) is a significant medical condition for women. This may open the door for companies to apply for new drug applications for that indication. It is important to note that unlike erectile dysfunction drugs approved for men, like Viagra, which increase blood flow to the genitals as long as a man is aroused, testosterone therapy is systemic and needs to be applied over weeks to have a noticeable effect on sex drive in men and women. Some companies have tried to enter the female sexual dysfunction market in the past. In December 2004, the United States FDA rejected Procter & Gamble's fast-track request for Intrinsa (a testosterone patch for women) for HSDD, citing concerns about potential off-label use of the product. In Canada, post-menopausal women have been able to obtain government-approved testosterone treatment since 2002. In 2007, Intrinsa was granted a license from the European Medicines Agency in July and was available on Britain's National Health Service. According to P&G's survey on female health, 30 million women in the U.S. are naturally menopausal, 3 million are distressed by their lack of sexual desire, and 20% of 25 million surgically menopausal women are distressed. Other companies that attempted to get their drugs approved for this indication (Boehringer Ingelheim and Warner Chilcott) have pulled the plug on their competing HSDD treatments for menopausal and pre-menopausal women. BioSante Pharmaceuticals also got their testosterone gel for women, LibiGel, rejected by the FDA. HORMONE THERAPY IN POSTMENOPAUSAL WOMEN Menopause can cause symptoms such as hot flashes that might result from the changing hormone levels during the menopause transition. After a woman's last menstrual period, when her ovaries make much less estrogen and progesterone, some symptoms of menopause might disappear, but others may continue. To help relieve these symptoms, some women use hormones. This is called hormone therapy (HT), which includes estrogen alone or in combination with progesterone. HT is available orally or in gel formulations made by specialized compounding pharmacies. Estrogen is a hormone used to relieve the symptoms of menopause. A woman who had her uterus removed could use only estrogen (E). But a woman with a uterus must add progesterone, or progestin (synthetic progesterone), and estrogen (E+P). This combination lowers the chance of an unwanted thickening of the uterus lining and reduces the risk of cancer of the uterus, an uncommon but possible result of using estrogen alone. CONTROVERSIES IN HORMONE TREATMENTS FOR WOMEN But the use of hormone therapy in women has been subject to much controversy in the recent past. The Women's Health Initiative (WHI) was a landmark clinical trial that looked at the effects of combination hormone therapy (estrogen + progestin) in 16,608 postmenopausal women with an intact uterus. The women were aged 50 to 79 (average age of 63) when they joined the study. This study did not include the use of testosterone. In this study, 8,506 participants were randomly assigned to receive a combination of estrogen (0.625 milligrams of conjugated equine estrogens per day) plus progestin (2.5 mg of medroxyprogesterone acetate), and 8,102 women were given a placebo. The study was stopped in 2002 after an average of 5.6 years of treatment due to increased breast cancer in women on hormone therapy. Compared to women on placebo, women on combination hormone therapy were also at increased risk of stroke, dangerous blood clots, and heart disease. In contrast, their risk of colorectal cancer and hip fractures was lower. It is important to note that these hormones were provided orally, and some clinicians claim that transdermal (on the skin) application of estrogen alone or in combination with testosterone would show a different and more favorable side effect profile. The halting of the WHI study raised concerns about the safety of all hormone therapy in women (oral or transdermal), even if no androgens were included in this study and only oral delivery forms were used. Many physicians stopped prescribing hormone therapy (HT) even for women who had dramatic improvements in their quality of life while using it. Experts today don't recommend hormone therapy unless a woman suffers painful menopause symptoms. New information about the use of androgens (testosterone and DHEA) alone or with HT suggests that these hormones may help women who do not have enough androgens and have problems with their sexual health. Androgens are also precursors of all estrogens (estrone (E1), estradiol (E2), and estriol (E3)) in women's bodies. The primary and most well-known androgen is testosterone (which aromatizes into estradiol); other less essential androgens are dihydrotestosterone (DHEA) and androstenedione. The ovaries and adrenals directly secrete androgens in women. Presently, there is no agreement about whether androgen deficiency is a clinical problem in aging women and if the addition of androgens to HT can improve the cardiovascular risks seen in the WHI study. Causes of androgen insufficiency in women can have ovarian, adrenal, hypothalamic-pituitary, drug-related, and unknown origins. Symptoms of adrenal insufficiency and androgen insufficiency in women may include a diminished sense of well-being, low mood, fatigue, and hypoactive sexual desire disorder (HSDD) with decreased libido or reduced sexual receptivity and pleasure that causes a great deal of personal distress. Premature ovarian insufficiency (POI) is another possible cause of androgen insufficiency in women. POI occurs when the ovaries stop functioning normally before 40 years of age. Although menopause is the most common cause of ovarian failure, other factors, such as chemotherapy or radiation therapy, can also contribute to POI. Therefore, it is important to consider premature ovarian insufficiency as a potential cause of androgen insufficiency in women. There is increasing evidence to suggest that many postmenopausal women experience symptoms alleviated by androgen therapy and that such symptoms may be caused by androgen deficiency. Affected women complain of fatigue, low libido, and diminished well-being, which are symptoms easily and frequently attributed to psychosocial and environmental factors. The question of whether adding testosterone therapy to conventional postmenopausal HT is effective or safe is unresolved. Therefore, a Cochrane review was performed to determine the efficacy and safety of testosterone therapy for postmenopausal women using HT. Thirty-five trials with a total of 4768 participants were included in the review. The median study duration was six months (range: 1.5 to 24 months). Most of the trials were of adequate quality regarding randomization. The pooled estimate suggested that adding testosterone to HT regimens improved sexual function scores and the number of satisfying sexual episodes for postmenopausal women. Some of the few adverse effects were decreased high-density lipoprotein (HDL) cholesterol levels and increased hair growth and acne incidence. The discontinuation rate was not significantly higher with the addition of testosterone therapy. OTHER USES FOR TESTOSTERONE IN WOMEN Emerging and controversial potential indications for androgen therapy in women have been or are being evaluated. Women with early ovarian failure, premenopausal androgen deficiency symptoms, postmenopausal and glucocorticosteroid-related bone loss, HIV-related wasting, and the premenstrual syndrome can all use this medicine. Whether or not any of these indications will lead to approved products in the future is unknown. HOW TO MEASURE LOW TESTOSTERONE IN WOMEN The term hypogonadism is used as a diagnostic term for testosterone deficiency, also known as testosterone insufficiency, in men. Besides HSDD as one of the potential symptoms, there is no agreement on what to call androgen deficiency in women. Clinical guidelines published in 2002 called the Princeton Consensus Statement used the term "female androgen insufficiency" as defined as a pattern of clinical symptoms in the presence of decreased bioavailable testosterone and normal estrogen status. The panel warned that currently available testosterone assays were found to lack sensitivity and reliability at the lower testosterone blood level ranges in women. The need for an equilibrium dialysis measure was strongly emphasized as the most adequate method to test women’s testosterone blood levels. BUY THE MOST AFFORDABLE AND ACCURATE TESTOSTERONE TEST FOR WOMEN Women in the United States can buy a testosterone test for women online without needing a doctor's prescription by using DiscountedLabs.com. They can also obtain a complete blood test panel to measure other hormones like estrogen, DHEA, progesterone, and testosterone. HOW TO TREAT LOW TESTOSTERONE IN FEMALES Circulating testosterone in women declines during the late reproductive years, such that otherwise healthy women in their 40s have approximately half the testosterone level as women in their 20s. The levels remain stable across the menopausal transition and then either remain stable or continue to decline with diminishing adrenal androgen production with increasing age. In the decade preceding menopause, the mid-cycle surge of free testosterone is lost. Despite this, research showing the benefits of androgen replacement has been limited to postmenopausal years. This means that testosterone levels in women change throughout the month based on one's menstrual cycle. However, the mid-cycle surge of free testosterone is lost in the decade preceding menopause. Some small studies have been done in premenopausal women, however. One evaluated the efficacy of transdermal testosterone therapy on mood, well-being, and sexual function in premenopausal women with low libido in eugonadal (normal testosterone blood levels). Testosterone therapy improved the well-being, mood, and sexual function of these women. Since many women experience diminished sexual interest and welfare during their late reproductive years, further research is warranted to evaluate the benefits and safety of the longer-term intervention. Potential dose-dependent side effects may be unwanted hair growth, masculinization, and high-density lipoprotein (HDL) lowering. TESTOSTERONE REPLACEMENT AND CARDIOVASCULAR RISKS IN WOMEN A direct association between testosterone and heart disease has never been established, but doctors have suspected a link exists for many years. The reasoning goes like this: men have much more testosterone than women and develop heart disease about ten years before their female counterparts. On top of standard medical therapy, women with systolic heart failure who took low-dose testosterone for six months showed significant gains in exercise and ventilatory capacity and large-muscle strength, along with heightened insulin sensitivity, in a small placebo-controlled trial . Despite the entrenched belief that higher blood levels of testosterone increase the risk of CVD in women, data from recent observational studies mostly show an inverse relationship between testosterone and CVD risk. A pilot study (JCEM 86 (1): 158) suggested favorable effects of transdermal testosterone treatment of women with established congestive cardiac failure, which merits further evaluation. Some early research shows that giving postmenopausal women testosterone therapy through injections improves both flow-mediated and GTN-mediated vasodilation in the brachial artery. The mechanisms underlying these potentially beneficial cardiovascular effects require further investigation. TESTOSTERONE REPLACEMENT AND CANCER IN WOMEN The relationship between endogenous testosterone production and breast cancer risk remains contentious, with recent studies indicating either no relationship or a possible increase in risk when estrone and estradiol are not considered. No randomized controlled trial of testosterone therapy has been sufficiently large or of sufficient duration to establish whether such treatment may influence breast cancer occurrence. There does not appear to be an association between testosterone and endometrial cancer or other malignancies in the review of published studies. There is no convincing evidence that standard estrogen-based hormone therapy for ovarian failure increases the risk of breast cancer. However, some studies have previously shown that ovarian androgens protect mammary epithelial cells from excessive estrogenic stimulation. Therefore, a study hypothesized that adding testosterone to usual hormone therapy might protect women from breast cancer. This retrospective observational study followed 508 postmenopausal women receiving testosterone and standard hormone therapy in South Australia. Breast cancer status was ascertained by mammography at the initiation of testosterone treatment and biannually after that. The average age at the start of follow-up was 56.4 years, and the mean duration of follow-up was 5.8 years. Breast cancer incidence in this group was compared with that of untreated women and women using usual hormone therapy reported in the medical literature and to age-specific local population rates. There were seven cases of invasive breast cancer in this population of testosterone users, for an incidence of 238 per 100,000 woman-years. The rate for estrogen/progestin and testosterone users was 293 per 100,000 woman-years—substantially less than women receiving estrogen/progestin in the Women's Health Initiative study (380 per 100,000 woman-years) or the Million Women Study (521 per 100,000 woman-years). The breast cancer rate in testosterone users in this study was closest to that reported for users who never used hormone therapy in the latter study (283 per 100,000 woman-years), and their age-standardized rate was the same as for the general population in South Australia. Based on these findings, adding testosterone to traditional hormone therapy for postmenopausal women may not raise the risk of breast cancer and may even lower it, bringing the rates back to what they are in the general population that is not on hormone therapy. But more studies are needed. LATEST DATA ON TESTOSTERONE AND WOMEN: A recent study review by Dr. Rakibul Islam and his team was published in The Lancet in July 2019 and retrieved 46 reports of 36 randomized controlled trials comprising 8480 female participants. Their meta-analysis showed that testosterone significantly improved sexual function compared to a placebo or a comparator (e.g., estrogen with or without progesterone). It improved sexual desire, pleasure, arousal, responsiveness, and self-image, and it decreased sexual concerns and distress in postmenopausal women. A significant rise in the amount of LDL-cholesterol and reductions in total cholesterol, HDL-cholesterol, and triglycerides were seen with testosterone administered orally but not when administered non-orally (e.g., by transdermal patch or cream). An overall increase in weight was recorded with testosterone treatment. No effects of testosterone were reported for body composition, musculoskeletal variables, or cognitive measures, although the number of women who contributed data for these outcomes was small. Testosterone was associated with a significantly greater likelihood of reporting acne and hair growth, but no serious adverse events were recorded. TESTOSTERONE USE IN WOMEN IN THE UNITED STATES As previously mentioned, there is no FDA-approved testosterone product for women. Some doctors prescribe drugs for female patients by having them use low doses of products like Androgen, Testim, Axiron, Testopel, and Fortesta that are meant for male hypogonadism without following the product's label. Other doctors prescribe creams with low testosterone levels through compounding pharmacies. However, it is important to note that women and people with AFIB require significantly less testosterone, necessitating a much lower dose of medication compared to men. CONCLUSION In conclusion, low testosterone in women is a condition that is often overlooked and underdiagnosed. However, it can have significant impacts on a woman's quality of life, including decreased sex drive, fatigue, and mood changes. Fortunately, there are several treatment options available, including hormone replacement therapy, lifestyle changes, and medication. It is important for women to speak with their healthcare provider and get properly diagnosed and treated for low testosterone if necessary. By doing so, they can improve their overall health and well-being. References: Effects of testosterone therapy for women: a systematic review and meta-analysis protocol.Syst Rev. 2019; 8: 19 Efficacy and safety of transdermal testosterone in postmenopausal women with hypoactive sexual desire disorder: a systematic review and meta-analysis. Fertil Steril. 2017; 107: 475-482 -
When is the best time to test for hormone imbalance in women?
Table of Contents Timing for Female Hormone Testing Female Hormone Testing Through Menstrual Cycle Women's Hormone Blood Testing Mistakes The Best Time for Female Hormone Blood Testing Female Hormone Testing Data Important Testing Precautions Reference Timing for Female Hormone Testing Throughout our life, male or female, many of us reach a point where things may not feel quite right. Our energy levels may be low; our desire for sexual activity is not what it used to be if it exists at all. We may be experiencing unexplained weight gain or muscle loss, not to mention issues with fertility. It is for these reasons; many men and women will seek out treatment options. Such options sought out by both sexes have increasingly been hormone treatment plans, which almost always begin with blood testing. This process is relatively more straightforward for most men, but female hormone testing is slightly more complicated. Timing for the female hormone blood panels is an essential factor that must be taken into consideration. Female Hormone Testing Through Menstrual Cycle When determining hormone levels within the body, a premenopausal woman requires blood tests that are timed for the most accurate results. You will find some labs, and physicians will offer saliva-based tests, which may not provide accurate results, but blood testing will often be the way to go for a fuller measure of various markers in the body. While the various tests are essential, blood testing itself must be coupled with appropriate timing. For example, for the adult male, generally, the best time to have blood drawn for testing is the first thing in the morning on an empty stomach. Some women may follow a similar approach, but for the female, this is far from optimal. Hormone testing for premenopausal women, our focus here today, is best timed around the woman's cycle. Depending on the specific hormone panel ordered, fasting for 12-14 hours may be necessary for comprehensive testing, but the female hormone blood test's timing needs further consideration around the menstrual cycle. Women's Hormone Blood Testing Mistakes Failure to time a blood test around a woman's cycle may render inaccurate hormone lab test results. One may find their hormone levels similar to a postmenopausal female even if still well within the premenopausal stage of life if the timing is off. For a healthy adult female with regular menstrual cycles, estrogen and progesterone blood test levels will be extremely low at the beginning of the follicular phase of one's cycle. These hormones will often mimic that of a menopausal female despite functioning ovaries. Any testing done during this period of a woman's cycle is useless. Although both men and women experience fluctuations in hormone levels throughout the day, week, and even months, more significant changes usually exist within a woman's monthly cycle. The Best Time for Female Hormone Blood Testing As menstrual cycle timing is crucial related to female hormone blood testing, most premenopausal women will find labs to be at their most accurate state at days 19-21 of their monthly cycle. This period is when they are at their peak production of progesterone. As alluded to before, progesterone will be lower during other points of the cycle to even seemingly nonexistent during the follicular stage. As many women supplement with progesterone, often for fertility purposes, one might ask how this would impact their choice in timing? If a woman is supplementing with medical progesterone, as it is usually only taken during the luteal phase of her cycle, which is when progesterone is sometimes only taken for fertility purposes; it is important to have blood work done at this point to view accurate results. As is with the woman who is not taking progesterone, we are merely attempting to test our hormone levels when progesterone is at its peak. It is important to note that some doctors prescribe testosterone for hormonal imbalances in women. However, suppose a low dose of progesterone does not accompany this exogenous testosterone. In that case, the testosterone treatment may negate the benefits of HRT since a therapeutic-created form of estrogen dominance will affect the quality of life. The introduction of a low dose of progesterone will help normalize the whole hormone gambit within the woman's body, thereby producing measurable results that can help her reach optimal health should treatments need adjustment. If you still have a menstrual cycle, the time of the month for estradiol and progesterone test is essential. Wrong timing will often render your lab result useless because, at certain times of the month, healthy women with normal and suboptimal hormone profile will have similar numbers to menopausal/peri-menopausal women. During the early follicular phase, estrogen and progesterone are naturally very low and in the menopausal range, even if you are a healthy 28-year-old with fully functioning ovaries and fertility. So, testing on the wrong days does not give you any useful data on your ovarian function. For women with 28-day cycles that ovulate on day 14, the best day to evaluate progesterone blood test levels is at its highest, seven days after ovulation. Female Hormone Testing Data A study published in 2006 reviewed the issue of timing of premenopausal hormone blood testing. It was a three-year study that included regular blood testing of 113 premenopausal women. The study performed estrogen and progesterone blood tests in both the luteal phase and the women's cycles' follicular phase. Data from the study showed that the differences between tests performed at the luteal and follicular phases were significant. Levels of free estradiol were the only marker of relative statistical insignificance. Estrogens and androgens, among other items, were statistically opposed between the two periods of testing, reinforcing the need for women to plan their hormone blood testing accordingly with their monthly cycle. While many women do not track their cycle, if blood testing is necessary and you are attempting to get to the bottom of an issue, tracking it is essential to make sense of female hormones' lab test results. Important Testing Precautions Before undergoing hormone testing, there are several important precautions to ensure accurate results: Biotin Interference: If you are taking biotin supplements (vitamin B7, B8, vitamin H, or coenzyme R), you should stop consumption at least 72 hours prior to blood collection, as biotin can interfere with many hormone tests and affect accuracy. Testosterone Cream Users: If you are using testosterone cream, ensure you have not applied any to the antecubital area (inner elbow area) of your arm for at least 24 hours before testing, as this can cause falsely elevated results. Fasting Requirements: Depending on your specific hormone panel, you may need to fast for 12-14 hours before blood collection. Fasting means no consumption of food or beverage other than water. Check with your testing provider about specific fasting requirements for your panel. If you find hormone testing is something you would like to do, a great place to start is with Discounted Labs' Women's Hormone Tests References Stacey A. Missmer, Donna Spiegelman, Elizabeth R. Bertone-Johnson, Robert L. Barbieri, Michael N. Pollak and Susan E. Hankinson. "Reproducibility of Plasma Steroid Hormones, Prolactin, and Insulin-like Growth Factor Levels among Premenopausal Women over a 2- to 3-Year Period." Cancer Epidemiol Biomarkers Prev. 2006 May;15(5):972-8. Prior JC (2020). "Women's reproductive system as balanced estradiol and progesterone actions—A revolutionary, paradigm-shifting concept in women's health". Drug Discovery Today: Disease Models. 32, Part B: 31–40. -
Does TRT Cause High Blood Pressure?
When it comes to TRT blood pressure, understanding the various factors that can impact this crucial health metric is essential for men who use testosterone. In this blog post, we'll talk about the link between testosterone replacement therapy (TRT) and high blood pressure, as well as some of the possible side effects and problems that may come up during treatment. We'll talk about the dangers of TRT-induced high blood pressure and emphasize how crucial regular monitoring is. Additionally, we'll examine water retention and edema in men on TRT, shedding light on their causes and management strategies. Furthermore, our investigation into testosterone's impact on kidney functioning will provide valuable insights into how hormone therapy affects renal function. We'll also debunk common misconceptions surrounding estrogen conversion's role in extracellular water (ECW) increases while exploring alternative explanations for changes in fluid balance during TRT. Lastly, we'll address lifestyle factors influencing water retention during hormone therapy, such as sodium intake, alcohol consumption's effects on fluid balance, and the significance of regular exercise throughout treatment. By gaining a deeper understanding of these issues related to TRT, blood pressure management becomes an achievable goal for those undergoing hormone therapy. Table of Contents: High Blood Pressure and TRT Risks Associated with High Blood Pressure Caused by TRT Importance of Regular Blood Pressure Monitoring Water Retention and Edema in Men on TRT Causes Behind Edema-Related Swelling in Men on TRT Strategies for Managing Water Retention The Importance of Cardiovascular Workup Testosterone's Impact on Kidney Functioning The Role Played by Kidneys in Regulating Body Fluids How Testosterone Affects Renal Function Taking Control of Blood Pressure During TRT Estrogen Conversion Not Responsible for ECW Increase Debunking Misconceptions about Estrogen's Role in ECW Increase Investigating Alternative Explanations for Changes in Fluid Balance Moving Forward: The Importance of Ongoing Research Lifestyle Factors Influencing Water Retention During TRT The Role of Sodium Intake in Water Retention Effects of Alcohol Consumption on Fluid Balance Importance of Regular Exercise During Hormone Therapy FAQs in Relation to Trt Blood Pressure Does TRT therapy raise blood pressure? Does testosterone play a role in blood pressure? Can testosterone cypionate cause high blood pressure? Does low testosterone shots cause high blood pressure? Conclusion High Blood Pressure and TRT Several studies have determined that having low testosterone may increase the incidence of high blood pressure in men. TRT can improve blood pressure control in hypogonadal men. However, in some other men, testosterone replacement therapy (TRT) can increase blood pressure during the initial weeks of treatment. Monitoring your blood pressure is crucial to regaining control over it while on TRT. In this section, we will discuss the dangers of TRT-related high blood pressure and emphasize the significance of regular blood pressure monitoring. Risks Associated with High Blood Pressure Heart Attacks: Elevated blood pressure puts extra strain on your heart muscles, which may eventually lead to heart attacks. When arteries become narrow due to plaque buildup or a clot forms in one of these vessels supplying oxygen-rich blood to your heart muscle cells, it could cause permanent damage. Strokes: High blood pressure can also cause strokes, which occur when there's an interruption in the flow of oxygenated blood supply towards specific regions within our brains, leading them to not be able to function properly anymore, resulting in either death, tissue loss, or, depending upon severity, the location of the affected area(s). Kidney Damage: Prolonged hypertension may result in chronic kidney disease (CKD) due to the increased workload placed on these organs, which filter waste products out of the bloodstream efficiently enough for elimination via the urine production process, eventually leading to renal failure if left untreated over time. Erectile Dysfunction: High blood pressure can cause erectile dysfunction by damaging the lining of your blood vessels and limiting the flow of blood to your penis. This makes it difficult for men to achieve or maintain an erection during sexual activity. Brain Shrinkage: Studies have shown that high blood pressure may contribute to a reduction in brain volume, also known as brain shrinkage. This condition has been linked with cognitive decline and an increased risk of dementia later in life. Importance of Regular Blood Pressure Monitoring To mitigate these risks while undergoing TRT, it is essential to monitor your blood pressure regularly if it is increasing. Here are some reasons why regular monitoring is crucial: Detecting Early Warning Signs: Frequent measurements help identify any fluctuations in your BP levels before they escalate into more severe health issues such as heart attacks or strokes, allowing you to take preventive measures early on. Maintaining an Optimal Treatment Plan: By keeping track of how well current medications work in controlling hypertension symptoms (if applicable), doctors are able to adjust dosages accordingly to ensure the best possible outcome for patients' overall wellbeing throughout the duration of therapy sessions undertaken using testosterone replacement products/services available in today's medical industry standards, practices, guidelines, and recommendations set forth by medical groups. Lifestyle Adjustments: Tracking changes allows individuals to pinpoint specific factors contributing to their elevated pressure - whether it be dietary habits, stress levels, or lack of exercise regimen adherence, among others; thus enabling them to make necessary adjustments in order to improve their overall health status while still receiving the benefits associated with TRT treatments being administered under the supervision of healthcare professional team members involved in the case management process. In conclusion, understanding the risks of high blood pressure caused by testosterone replacement therapy and monitoring your BP regularly is essential for maintaining optimal health during treatment. By making lifestyle adjustments and working closely with your healthcare provider, you can effectively manage hypertension while reaping the benefits of TRT. Key Takeaway: In some men with metabolic syndrome, older age, and other factors, testosterone replacement therapy (TRT) can increase blood pressure, which poses long term risks such as heart attacks, strokes, kidney damage, erectile dysfunction, and brain shrinkage. Monitoring and treating your blood pressure is crucial to regain control over it while on TRT, and making lifestyle adjustments with the help of healthcare providers can effectively manage hypertension while reaping the benefits of TRT. Water Retention and Edema in Men on TRT One potential side effect of testosterone therapy is edema, particularly dependent edema, which is more common in older men [10]. Edema refers to water retention, and dependent indicates water retention towards the ground, such as when sock imprints are visible around the ankles after removing them. Testosterone-induced water retention can cause swelling in the extremities, particularly in the legs and feet, leading to discomfort and potential complications if left untreated. A study looking at various doses of testosterone enanthate in older men revealed nearly half experienced leg edema in the groups provided with supraphysiologic testosterone (300 and 600 milligrams per week of testosterone enanthate). A comprehensive cardiovascular workup may help identify any underlying issues contributing to this condition, while maintaining a low-sodium diet and drinking plenty of water can alleviate symptoms. In this section, we will discuss the causes behind edema-related swelling in men on TRT and strategies for managing water retention. Causes Behind Edema-Related Swelling in Men on TRT The primary cause of edema-related swelling during TRT is an increase in extracellular fluid volume resulting from testosterone's impact on sodium reabsorption in the kidneys. Testosterone stimulates sodium and water retention through an autocrine or paracrine mechanism that affects sodium metabolism, leading to elevated blood pressure levels experienced by some men undergoing hormone therapy. Men with pre-existing metabolic syndrome, obesity, baseline high blood pressure, and kidney dysfunction can be more susceptible than others to having this problem. Additionally, certain lifestyle factors, such as high sodium intake, alcohol consumption, and a lack of exercise, can exacerbate these symptoms. Strategies for Managing Water Retention To minimize the impact of TRT-induced edema and improve overall health outcomes, it is essential to adopt effective management strategies targeting both hormonal imbalances caused by treatment itself as well as lifestyle factors that contribute to fluid accumulation within the body: Maintain a Low-Sodium Diet: Reducing your daily salt intake helps prevent excessive fluid buildup around cells, which could lead to hypertension. Aim for less than 2300 mg per day, according to CDC guidelines. Stay Hydrated: Drinking adequate amounts of water helps flush out excess sodium and promotes healthy kidney function. Aim for at least eight 8-ounce glasses per day, or consult your healthcare provider for personalized recommendations based on individual needs. Incorporate Regular Exercise: Engaging in regular physical activity not only aids weight management but also improves circulation and reduces fluid retention. Choose activities that you enjoy, such as walking, swimming, or cycling, to maintain consistency. Minimize Alcohol Consumption: Alcohol can dehydrate the body and increase water retention by disrupting hormonal balance. Limiting alcohol intake will help minimize edema-related swelling during TRT. Monitor Blood Pressure Regularly: Keeping track of your blood pressure levels is crucial to ensuring they remain within a healthy range while undergoing hormone therapy. Invest in a reliable home blood pressure monitor and take readings daily until control is regained. Besides these strategies, it's essential to communicate with your healthcare provider about any concerns related to edema or other side effects experienced during TRT. They may recommend adjustments in dosage or additional medications such as diuretics (water pills), which aid in reducing fluid buildup within the body, if necessary. Physicians may also recommend lowering the TRT dose or switching from testosterone injections to gels to attain lower testosterone blood level peaks. The Importance of Cardiovascular Workup If you are experiencing persistent edema-related swelling despite implementing the above strategies, it might be time for a comprehensive cardiovascular workup conducted by a qualified medical professional specializing in men's health issues like testosterone deficiency (hypogonadism). A qualified medical professional specializing in men's health issues such as testosterone deficiency (hypogonadism) can perform a comprehensive cardiovascular workup to assess any underlying heart or vascular issues that may be contributing to fluid retention. In conclusion, managing water retention during TRT is crucial for maintaining optimal health outcomes while undergoing hormone therapy. By adopting effective strategies targeting both hormonal imbalances caused by treatment itself as well as lifestyle factors that contribute to fluid accumulation within the body, men on TRT can minimize edema-related swelling and improve their overall quality of life. Key Takeaway: Due to the effect of testosterone on kidney function, men receiving testosterone replacement therapy (TRT) may experience swelling associated with edema. To manage this side effect, men should maintain a low-sodium diet, stay hydrated, exercise regularly, minimize alcohol consumption, and monitor their blood pressure levels. If these strategies do not work, it is important to seek a comprehensive cardiovascular workup from a qualified medical professional specializing in men's health issues like hypogonadism. Testosterone's Impact on Kidney Functioning Increased extracellular water retention, which is a result of testosterone's impact on kidney function, may be the cause of elevated blood pressure levels in men undergoing TRT. One possible explanation for this phenomenon is the direct impact of testosterone on the way kidneys manage sodium in the body. In this section, we will explore the role played by kidneys in regulating body fluids and how testosterone affects renal function. The Role Played by Kidneys in Regulating Body Fluids Kidneys play a crucial role in maintaining overall health by filtering waste products from the bloodstream and excreting them as urine. Additionally, these vital organs are responsible for balancing electrolytes such as sodium and potassium while also controlling fluid balance within the body. This process involves adjusting both water intake through thirst signals and water output via urine production based on factors like hydration status, blood pressure levels, and hormone regulation. A key component of kidney function is its ability to regulate extracellular fluid volume (ECFV), which includes both interstitial fluid surrounding cells and plasma within blood vessels. ECFV directly impacts blood pressure since it determines the amount of circulating blood volume that needs to be pumped throughout the body by the heart. How Testosterone Affects Renal Function The primary effect of testosterone on the kidneys is the stimulation of sodium reabsorption. This means that the kidney cells are instructed to retain more sodium, which can lead to an increase in blood pressure. This is one of the reasons why testosterone replacement therapy is not recommended for men with hypertension unless blood pressure is managed first. Research has shown that testosterone could act directly on the kidneys through an autocrine or paracrine mechanism, stimulating sodium reabsorption along with increased water retention. This effect leads to a higher extracellular fluid volume, resulting in elevated blood pressure levels experienced by some men undergoing hormone therapy. Autocrine mechanism: Testosterone may act directly on the kidney cells that produce it, leading to an increase in sodium and water reabsorption. This process can contribute to elevated blood pressure levels by increasing extracellular fluid volume. Paracrine mechanism: Testosterone could also influence neighboring kidney cells through paracrine signaling, which involves the release of chemical messengers that travel short distances to affect nearby cells. In this case, testosterone might stimulate adjacent renal tubule cells responsible for regulating sodium and water balance within the body. In addition to these direct effects on kidney function, testosterone has been shown to impact other hormones involved in fluid regulation, such as aldosterone and vasopressin. For example, studies have found that men with low testosterone levels exhibit reduced aldosterone secretion, a hormone responsible for promoting sodium retention and potassium excretion by the kidneys. Consequently, when TRT is administered and testosterone levels rise again, there could be an associated increase in aldosterone production, resulting in greater sodium retention along with increased extracellular fluid volume. Taking Control of Blood Pressure During TRT If you are experiencing high blood pressure while undergoing TRT due to increased extracellular water retention caused by changes in renal function, hormonal imbalances related to treatment itself, or lifestyle factors like diet and exercise habits (as discussed earlier), it's essential to take proactive steps towards managing your condition effectively: Maintain regular check-ups with your healthcare provider. Your doctor will monitor your progress during TRT closely so they can adjust dosage if necessary or recommend additional interventions such as medication adjustments or lifestyle modifications aimed at reducing blood pressure levels. Monitor your blood pressure at home: Invest in a reliable home blood pressure monitor and take readings twice daily to keep track of any fluctuations that may occur during treatment. Maintain a healthy lifestyle: incorporate regular exercise, good hydration, a balanced diet low in sodium, limit alcohol consumption, and manage stress levels to help minimize the impact of TRT on blood pressure and overall health. In conclusion, understanding how testosterone impacts kidney function can provide valuable insights into managing high blood pressure during hormone therapy. By taking proactive steps towards maintaining optimal renal health while undergoing TRT, men can experience the benefits of this treatment without compromising their cardiovascular well-being. Key Takeaway: Testosterone replacement therapy (TRT) can lead to an increase in extracellular water retention, which contributes to elevated blood pressure levels. Testosterone impacts kidney function by stimulating sodium reabsorption and increasing water retention, resulting in a higher extracellular fluid volume that causes high blood pressure. To manage this condition effectively, it's essential to maintain regular check-ups with your healthcare provider, monitor your blood pressure at home, and maintain a healthy lifestyle. Estrogen Conversion May Not Be Responsible for Water Retention It was once believed that the increase in extracellular water (ECW) experienced by men undergoing testosterone replacement therapy (TRT) could be attributed to the conversion of testosterone into estrogen within peripheral tissues. However, recent research has debunked this hypothesis, indicating that other mechanisms must be at play when it comes to understanding how hormone treatments impact fluid balance within the body. In this section, we will explore why estrogen is not responsible for increased ECW and discuss alternative explanations for changes in fluid balance during TRT. Debunking Misconceptions about Estrogen's Role in ECW Increase The idea that estrogen might be responsible for increased ECW stemmed from its known effects on sodium and water retention. Indeed, studies have shown that elevated levels of estrogen can lead to an increase in total body water due to enhanced renal reabsorption of sodium and subsequent water retention. This led some researchers to speculate whether a similar mechanism might explain the observed rise in extracellular fluid volume among men receiving TRT. However, more recent investigations have demonstrated no significant correlation between circulating estradiol levels (the primary form of estrogen) and changes in extracellular fluid volume following testosterone administration. These findings imply that the aromatization, or conversion, of testosterone into estradiol cannot solely account for any increase in ECW experienced by men on TRT. Investigating Alternative Explanations for Changes in Fluid Balance In light of these discoveries, scientists are now considering other potential mechanisms that might account for the increase in ECW observed among men undergoing hormone therapy. One such possibility is that testosterone itself may directly affect kidney function, as discussed earlier in this article. Due to its modulation of secretion and action, testosterone levels may have an impact on vasopressin, a hormone that regulates the body's water balance. Recent studies suggest that testosterone can also modulate vasopressin secretion. Vasopressin is a hormone that regulates water balance and blood pressure in the body. It is released from the pituitary gland and acts on the kidneys to regulate the amount of water excreted in urine. Research shows that testosterone can regulate the production and release of vasopressin in the hypothalamus, a region of the brain that plays a key role in regulating hormone secretion. Testosterone can enhance vasopressin secretion, which in turn can increase water reabsorption in the kidneys and reduce urine output. Therefore, testosterone can have an impact on the body's fluid balance, which can have implications for overall health and well-being. More research is needed to fully understand the complex relationship between testosterone and vasopressin secretion. A third hypothesis involves aldosterone, another hormone involved in maintaining proper electrolyte balance and blood pressure regulation.Testosterone has been found to stimulate aldosterone production, which could theoretically contribute to changes in ECW by promoting sodium retention and subsequent water reabsorption at the level of renal tubules. Another factor that may increase blood pressure is the effect of TRT on increasing red blood cells and hematocrit to high levels in some men. High hematocrit can increase blood viscosity and blood pressure. In addition to these hormonal factors, it's important not to overlook lifestyle influences when examining changes in fluid balance during TRT. As mentioned previously, high-sodium diets, alcohol consumption, and a lack of exercise can all exacerbate water retention issues among men receiving hormone treatments. Moving Forward: The Importance of Ongoing Research While we now know that estrogen conversion is not responsible for increased ECW during TRT, there remains much work to be done when it comes to understanding how various factors influence fluid balance among individuals undergoing this form of therapy. Continued research into hormonal pathways - as well as individual differences related to both genetics and lifestyle choices - will help paint a clearer picture regarding how to best manage side effects like edema-related swelling while optimizing the overall benefits of TRT for men who need it. For now, it's essential that patients and healthcare providers alike remain vigilant when monitoring fluid balance during hormone therapy. By staying informed about the latest research findings and being proactive in addressing any potential issues related to water retention, men on TRT can minimize their risk of experiencing complications while maximizing the positive impact of treatment on their health and well-being. Key Takeaway: Recent research has debunked the hypothesis that estrogen is responsible for increased extracellular water (ECW) in men undergoing testosterone replacement therapy (TRT). Alternative explanations include direct effects of testosterone on kidney function, modulation of vasopressin secretion and action, and stimulation of aldosterone production. It's important to monitor fluid balance during hormone therapy and consider lifestyle influences such as high-sodium diets, alcohol consumption, and a lack of exercise. Lifestyle Factors Influencing Water Retention During TRT Men receiving testosterone replacement therapy (TRT) may experience increased water retention when consuming high-sodium foods, drinking alcohol, or skipping gym sessions for more than three days. Adjusting these lifestyle factors can help minimize the impact of TRT on blood pressure and fluid balance. The Role of Sodium Intake in Water Retention A diet high in sodium can cause your body to retain more water, leading to an increase in extracellular fluid volume. This is particularly true for men undergoing testosterone replacement therapy, as their bodies are already prone to retaining excess fluids due to the hormonal changes taking place. To combat this issue, it's essential that you monitor your daily sodium intake while on TRT. Limit processed foods: Processed and packaged foods often contain large amounts of hidden sodium. Opt for fresh fruits, vegetables, lean meats, and whole grains instead. Cook at home: Preparing meals at home allows you greater control over the amount of salt used in your dishes. Experiment with herbs and spices to add flavor without relying on salt. Read food labels: Pay attention to the nutritional information provided on food packaging so you're aware of how much sodium each product contains. Avoid dining out frequently: Restaurant meals tend to be higher in sodium compared to homemade options; limit eating out whenever possible. Effects of Alcohol Consumption on Fluid Balance In addition to increasing overall caloric intake and potentially contributing to weight gain, alcohol consumption can also have a negative impact on fluid balance in men undergoing TRT. Alcohol acts as a diuretic, causing your body to lose fluids and electrolytes through increased urine production. This loss of fluids can lead to dehydration, which may exacerbate blood pressure issues and water retention problems associated with testosterone therapy. To minimize the effects of alcohol on fluid balance during TRT: Limit alcohol intake: Aim for moderate drinking habits by consuming no more than two alcoholic beverages per day for men. Stay hydrated: Drink plenty of water throughout the day and especially when consuming alcohol to counteract its dehydrating effects. Avoid binge drinking: Consuming large amounts of alcohol in a short period increases the risk of dehydration and worsens blood pressure and water retention problems related to TRT. Importance of Regular Exercise During Hormone Therapy Maintaining an active lifestyle is crucial for overall health and well-being while undergoing hormone therapy. Regular exercise not only helps control weight gain but also plays a vital role in managing blood pressure levels and promoting healthy circulation. Additionally, physical activity has been shown to help reduce edema-related swelling caused by excess extracellular fluid buildup - one common side effect experienced by many men receiving testosterone treatment. Incorporate these tips into your fitness routine while on TRT: Create a consistent schedule: Aim for at least three days per week dedicated to cardiovascular exercises such as brisk walking, jogging, or swimming; consistency is key when it comes to maintaining optimal blood pressure levels during hormone therapy treatments like TRT. Incorporate strength training: Building muscle mass can help improve arterial stiffness and reduce the risk of cardiovascular disease and heart attacks. Monitor progress: Keep track of your progress and adjust your exercise routine as needed to ensure you're getting the most out of your workouts. Key Takeaway: Men undergoing testosterone replacement therapy (TRT) may experience increased water retention due to hormonal changes, which can impact blood pressure. To minimize the effects of TRT on fluid balance, it's important to monitor sodium intake, limit alcohol consumption, and maintain a regular exercise routine that includes both cardiovascular exercises and strength training. FAQs in Relation to TRT and Blood Pressure Does TRT therapy raise blood pressure? TRT therapy can potentially raise blood pressure in some individuals, especially if they have pre-existing hypertension or other cardiovascular risk factors. However, the effect varies from person to person and depends on individual health conditions and lifestyle factors. Regular monitoring of blood pressure is essential during TRT. Does testosterone play a role in blood pressure? Testosterone does play a role in regulating blood pressure by influencing vascular function, kidney function, and body fluid balance. However, its impact on an individual's blood pressure may vary depending on various factors such as age, overall health status,the presence of pre-existing metabolic syndrome or cardiovascular issues, hormone levels, and lifestyle choices. Can testosterone cypionate cause high blood pressure? Testosterone cypionate is a form of injectable testosterone used for TRT. It has the potential to cause high blood pressure in some men due to increased water retention or changes in renal function associated with higher testosterone levels. Monitoring your BP regularly while using this medication is important. Does low testosterone shots cause high blood pressure? Low-testosterone shots are typically administered as part of TRT when treating hypogonadism (low T). These injections can sometimes lead to elevated BP due to increased water retention or altered kidney functions; however, it doesn't happen universally among all patients undergoing treatment. Maintaining healthy habits like exercising regularly and reducing sodium intake will help mitigate the risks associated with elevated blood pressure. Conclusion Therefore, it is essential to monitor blood pressure regularly in order to avoid potential cardiovascular complications associated with TRT. Regular monitoring of blood pressure is crucial to preventing cardiovascular disease and other related health issues. While TRT can have a positive impact on muscle mass and metabolic syndrome, it's important to manage any side effects that may arise. If you're interested in learning more about the role of the pituitary and thyroid in the diagnosis and treatment of TRT blood pressure, check out this informative article from Testosterone Wisdom. Take control of your health today by educating yourself on the benefits and risks associated with TRT blood pressure management! -

Testosterone Replacement Therapy: Products and Costs
Categories: Testosterone Doctor , Testosterone Tests , Testosterone Side Effect Management , TRT Side Effects , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , TRT Monitoring , TRT Guidelines , Testosterone Replacement Monitoring Tests , Free Testosterone TestDid you know that testosterone deficiency has a prevalence of up to 40% in adult males in the United States? A man is deficient in testosterone when his T levels fall below 300 ng/dL of blood. Although this is slightly worrisome news, there are multiple testosterone replacement options you can take advantage of these days. This article focuses on some of the most important testosterone products in 2023. Keep reading to learn key facts, statistics, price ranges, and optimal dosages related to your favorite testosterone products. Top Testosterone Replacement Therapy Options You Have in 2023 Fortunately, there are many ways you can get more testosterone into your system. There are patches, pellets, gels, injections, and even oral capsules that you can take once or twice a day. If you don't really fancy having to inject testosterone once a week, you can take capsules orally and reap all the benefits of testosterone replacement therapy. The following is a quick list of testosterone replacement products you can take advantage of to increase blood T levels. Administration of T products should only be done according to the strict guidance of your TRT doctor. FDA-Approved Testosterone Brands Androderm: Androderm is a transdermal testosterone patch that delivers testosterone through the skin. It is applied daily to maintain stable testosterone levels in men with low testosterone due to certain medical conditions[1]. This option is no longer used by most doctors since its efficacy was not good and it caused skin irritation. AndroGel: AndroGel is a topical testosterone gel that is applied directly to the skin, typically on the upper arms, shoulders, or abdomen. It is designed for daily use to help maintain consistent testosterone levels for men with low testosterone[1]. It comes in two concentrations. Fortesta: Fortesta is another topical testosterone gel applied to the skin, usually on the front and inner thighs. It is used for testosterone replacement therapy in males with low testosterone levels[2]. Testim: Testim is a testosterone gel applied daily to the skin, typically on the upper arms and shoulders, to help maintain consistent testosterone levels in men with low testosterone due to certain medical conditions[1]. Depo-Testosterone: Depo-Testosterone is an injectable form of testosterone prescribed for men with low testosterone levels. It is administered by a healthcare professional at regular intervals, typically every two to four weeks[2]. Testopel is a subcutaneous testosterone pellet that a medical professional implants under the skin. The pellets release testosterone over an extended period, typically three to six months[2]. Aveed: Aveed is an injectable testosterone undecanoate solution designed for long-acting testosterone replacement therapy. It is administered by a healthcare professional at regular intervals, typically every 10 weeks after an initial loading phase[2]. Natesto: Natesto is a testosterone nasal gel that is applied inside the nostrils for testosterone replacement therapy. It is used to treat men with low testosterone levels due to certain medical conditions[2]. Vogelxo: Vogelxo is a topical testosterone gel applied daily to the skin, usually on the upper arms, shoulders, or abdomen. It is used for testosterone replacement therapy in males with low testosterone levels[2]. Xyosted: Xyosted is a subcutaneous testosterone enanthate autoinjector for weekly self-administration. It is prescribed for men with low testosterone levels due to certain medical conditions[2]. Jatenzo: Jatenzo is an oral testosterone undecanoate capsule that the FDA has approved to treat certain types of hypogonadism in men. It is taken orally to help maintain stable testosterone levels in men with low testosterone [2] Testosterone Treatment Prices and Dosing Androgel 1% Price for a 30-day supply (in USD): 55-85 for the generic pump, 90-190 for 50 mg generic packets; also, around 650 USD for Brand 50 mg packets Delivery mode: pump and/or packet Dosage: 25 mg/2.5 g or 50mg/5g Where to apply shoulders, upper arms or on the abdomen Starting dosage: 50 mg daily dose early in the morning When to measure: in the morning before applying the gel Androgel 1.62% Price for a 30-day supply (in USD): 40-140 for the generic pump, 620-640 for Brand pump Delivery mode: pump and/or packet Dosage: 20.25 mg or 40.5 mg Where to apply shoulders or upper arms Starting dosage: 40.5 mg daily dose early in the morning When to measure in the morning before applying the gel Testim 1% Price for a 30-day supply (in USD): around 600-610 for packets Delivery mode: pump Dosage: 20.25 mg per actuation Where to apply shoulders or upper arms Starting dosage: one pump on each shoulder for a total of 40.5 mg early in the morning, it can also be applied on inner thighs When to measure: in the morning before applying the gel Fortesta 2% Delivery mode: pump Dosage: 50 mg or 100 mg Where to apply shoulders or upper arms Starting dosage: two pumps daily in the morning on each thigh When to measure: 2 hours after applying a dose Vogelxo Price for a 30-day supply (in USD): 100-350 for 1% pump, 120-350 for generic packets Delivery mode: shoulders or upper arms Dosage: 50 mg from 4 actuations of 12.5 mg testosterone Where to apply shoulders or upper arms Starting dosage: 50 mg daily in the morning When to measure before applying a dose Androderm Delivery mode: patch applied at night after 10 PM Dosage: 2 mg per day, 2.5 mg per day, 4 mg per day or 5 mg per day Where to apply: abdomen, upper arms, thighs, back Starting dosage: 4 mg per day When to measure: 12 hours after skin application Natesto Price for a 30-day supply (in USD): 195-300 for 5.5 mg/actuation Delivery mode: intranasal pump Dosage: 5.5 mg per pump actuation Where to apply intranasal Starting dosage: 11 mg (2 actuations) 3 times per day at an interval of 6-8 hours When to measure: 2 hours after nasal application Jatenzo Price for a 30-day supply (in USD): around 950 for 237 mg BID pill Delivery mode: oral capsule Dosage: 158 mg, 198 mg, or 237 mg Where to apply oral Starting dosage: 237 mg capsule twice a day (one in the morning, one in the evening) When to measure: 6 hours after the morning dose Testopel Delivery mode: pellet Dosage: 75 mg per pellet Where to apply can be inserted under the skin, in the fat of the buttocks, thigh or lower abdominal wall Starting dosage: 150-450 mg every 3 to 6 months When to measure: at the end of the dosing interval Aveed Delivery mode: injectable solution Dosage: 100 mg/10 ml vial, 200 mg/1-10 ml vial or 750 mg/3 ml vial Where to apply: intramuscular in the glute or thigh muscles Starting dosage: 750 mg (3 ml) in the beginning, then after 4 weeks then after every 10 weeks; 75-100 mg/week also or 150-200 mg every 2 weeks When to measure: injections are administered every 10 weeks and T measurement should be done somewhere in between injections (after 5 weeks or so since the last one) Xyosted Price for a 30-day supply (in USD): 455-575 for 50 mg, 75 mg and 100 mg injections Delivery mode: the solution is placed in the autoinjector Dosage: 50 mg, 75 mg or 100 mg respectively Where to apply: in the abdominal region under the skin Starting dosage: 75 mg applied under the skin once a week When to measure T levels: trough concentrations are measured 7 days after the most recent dose and only after 6 weeks since the beginning of treatment. These are just a few popular testosterone replacement products available in the US. Keep in mind that you can also procure testosterone enanthate in 5 ml (1000mgs) vials from certain pharmacies. This option usually costs less than $30 for a 30-day supply and the testosterone can be injected by each patient without requiring a doctor's visit. Similarly, TRT patients can also choose to use generic testosterone cypionate or enanthate as 400 mg to 800 mg per month that can be injected into muscle (deep IM or shallow IM) or under belly fat (subcutaneous) . The price for a 30-day supply starts at around $30 and it can go up to $85 . (Source: GoodRx). Other affordable sources of testosterone treatments can be purchased from compounding pharmacies like Empower in Houston. Check Out How AUA and ES Guidelines Differ on Testosterone Ranges AUA stands for American Urology Association and ES stands for Endocrine Society. They provide detailed insights and standards on how to interpret hormone levels and blood test results. In some cases, these committees can give different interpretations when it comes to testosterone levels. AUA Guidelines: What is a Normal Testosterone Range and Follow Up? According to the American Urology Association (AUA), you should measure your testosterone levels in the morning after fasting for 12-14 hours to get accurate results. The normal range is between 450 ng/dL and 600 ng/dL of blood. If your levels fall below 300 ng/dL of blood, you are considered to be deficient in testosterone. If you start testosterone replacement therapy, your first evaluation should be between 2 and 4 weeks after beginning treatment. You will also have to attend follow-up visits 6 to 12 months after starting TRT. ES Guidelines: What is a Normal Testosterone Range and Follow Up? On the other hand, the Endocrine Society (ES) gives slightly different reference ranges. For example, the normal testosterone range is between 264 ng/dL and 916 ng/dL of blood. The best moment to test your T levels is early in the morning after fasting for 12-14 hours. Testosterone deficiency is confirmed if your T levels fall below 264 ng/dL of blood. TRT follow up visits should be done after 2-3 months and after 6 to 12 months from the start of your testosterone replacement protocol. How to Get Your Own Affordable Testosterone Test Remember that now it's easier than ever to check your testosterone levels and see if you are a suitable candidate for testosterone replacement therapy. If your T levels fall below 350 ng/dL and have low testosterone symptoms then you should talk with a TRT doctor and see what testosterone replacement options you have. Check your testosterone levels quickly and confidentially by ordering a total and free testosterone test from DiscountedLabs today. Key Terminology and Facts About Testosterone It's important to also have some basic understanding of how testosterone works in the body, so you can make better decisions when talking with your TRT doctor. For instance, the Leydig cells in your testicles produce more than 95% of your testosterone. Testosterone daily production ranges from 3 mg to 11 mg and it peaks early in the morning. Healthy adult males have the highest concentration of testosterone early in the morning and it gradually drops throughout the day. That's why the best time to measure your T levels is early in the morning to get accurate results. Natural Testosterone Short half-life - your testosterone has a half-life between 10 and 100 minutes. It peaks once every 3 hours as the luteinizing hormone stimulates the Leydig cells to produce more testosterone. With the passing of time, these cells become less sensitive to LH and they produce increasingly low T levels. It's estimated that males lose about 1% of their testosterone production every year after the age of 30. 2 percent is free; about 2% of your total testosterone level is free. This means that it circulates freely through the bloodstream and it can bind to other organs or tissues. 70% of your testosterone is bound to sex hormone-binding globulin and nearly 30% is bound to albumin. Testosterone metabolism - fractions of your testosterone are converted into other hormones and substances. For example, from 5% to 8% of your testosterone is converted into dihydrotestosterone (DHT). This hormone is responsible for prostate maturation and the growth of the body, as well as facial and pubic hair. About 0.3%–0.5% of your testosterone is also converted into estradiol by the aromatase enzyme. Some of the main roles of estradiol in men are involved with libido and bone health. Trough concentration - this refers to the lowest concentration of a drug in the bloodstream immediately before injecting or administering another dose. It's highly recommended to measure your testosterone levels at trough concentration because this will produce the most accurate results. Based on these results, TRT doctors can make more accurate adjustments to your protocol. Find Out More About Testosterone Products! This is just a brief overview of some of the most popular testosterone products in the US, but there's plenty more high-quality information out there. Visit Excelmale.com and learn everything you need to know about testosterone, TRT, how to interpret your blood test data, and how to tweak your protocol for optimal results. Also, you can download the Testosterone Replacement Options paper from this link. References: [1] "FDA-approved testosterone formulations include the topical gel, transdermal patch, buccal system (applied to upper gum or inner cheek), and injection. The manufacturers of two prescription..." URL: https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/testosterone-information [2] "by Drugs.com Brand names of testosterone include Androderm, AndroGel, Fortesta, Testim, Depo-Testosterone, Testopel, Aveed, Natesto, Vogelxo, Xyosted, Jatenzo, Tlando, and Kyzatrex. Testosterone is an androgen indicated for testosterone replacement therapy in males." URL: https://www.drugs.com/medical-answers/brands-testosterone-3510863/ Recommended Sources: Testosterone Replacement Therapy Options | Excel Male TRT Forum Testosterone Replacement Products in the U.S.: Video Review by Nelson Vergel - ExcelMale Testosterone Test Near Me: Your Complete Guide Testosterone levels show steady decrease among young US men -
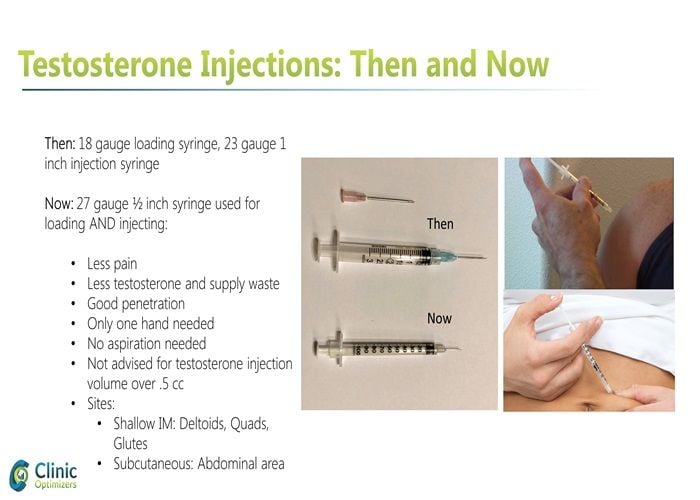
Where to Inject Testosterone: Intramuscular vs. Subcutaneous Injections
Categories: Testosterone Tests , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , TRT Monitoring , Testosterone in Women , Bodybuilder Blood WorkTestosterone Injection: Subcutaneous vs. Intramuscular—Where to Inject Regardless of which TRT product you’ve been prescribed, a common question is where to inject testosterone. For decades, most men have used IM testosterone injections, primarily into the glutes, quads, or deltoids, using a 1 to 1.5-inch syringe. During the past five years, many men have also begun injecting testosterone subcutaneously (SubQ), a shallow injection into the fat layer on the abdominal or other areas—just under the skin but before reaching muscle. Many TRT patients find SubQ injections less bothersome than IM injections, as they require a smaller needle in both length and gauge. SubQ injections are also associated with less irritation for some men with IM injections. While some men may find IM injections to leave a minor soreness at the injected site, SubQ injections cause no noticeable pain or irritation. Understanding Testosterone Replacement Therapy Testosterone Replacement Therapy (TRT) is a medical treatment designed to help individuals with low testosterone levels, also known as hypogonadism. TRT aims to restore normal testosterone levels, alleviating symptoms such as low libido, fatigue, and decreased muscle mass. This form of hormone therapy can significantly improve the quality of life for those experiencing sexual dysfunction and other related issues. TRT can be administered through various methods, including intramuscular injections, subcutaneous injections, and topical gels. In this article, we will focus on testosterone injections, specifically intramuscular and subcutaneous injections, to provide a comprehensive understanding of these methods. Testosterone Injection Methods: Effects on Total Testosterone, Estradiol (E2), and PSA Testosterone Cypionate and Testosterone Enanthate are the two most commonly used forms of testosterone in men to treat hypogonadism (low testosterone). Both forms carry the same testosterone hormone; the ester is the only difference, which alters the hormone’s time release so that testosterone blood levels can remain up for a few days. These two testosterone compounds are identical in a testosterone replacement therapy (TRT) setting. Both forms are commonly used in hormone replacement therapy to treat hypogonadism in men. Where and How to Inject Testosterone? Regardless of which TRT product you’ve been prescribed, a common question is where to inject testosterone. For decades, most men have injected their testosterone intramuscularly (IM), primarily into the glutes, quads, or deltoids, using a 1- to 1.5-inch syringe. During the past five years, many men have also begun injecting testosterone subcutaneously (SubQ), a shallow injection into the fat layer on the abdominal or other areas—just under the skin but before reaching muscle. Many TRT patients find SubQ injections less bothersome than IM injections, as they require a smaller needle in both length and gauge. SubQ injections are also associated with less irritation for some men with IM injections. While some men may find IM injections to leave a minor soreness at the injected site, SubQ injections cause no noticeable pain or irritation. Many patients find it beneficial to inject weekly to maintain stable testosterone levels. Administering Testosterone Injections Safely Administering testosterone injections safely requires proper technique and precautions to ensure effectiveness and minimize risks. Before injecting, ensure the injection site is clean and free of any debris. Use a sterile needle and syringe, and follow the recommended dosage and injection frequency as prescribed by your healthcare provider. For intramuscular injections, use a longer needle (1 to 1.5 inches) and insert it at a 90-degree angle into the muscle, typically in the glutes, quads, or deltoids. For subcutaneous injections, use a shorter needle (0.5 to 1 inch) and insert it at a 45-degree angle into the fatty tissue, commonly in the abdominal area. Always dispose of used needles and syringes properly to prevent injury and contamination. By following these steps, you can administer testosterone injections safely and effectively. Choosing the Right Injection Site Choosing the right injection site is crucial for safe and effective testosterone injections. For intramuscular injections, common sites include the buttocks, thigh, and upper arm. These areas have larger muscle masses, which are ideal for proper absorption of the hormone. For subcutaneous injections, common sites include the abdomen, thigh, and buttock. When selecting an injection site, consider the following factors: Fat layer: Subcutaneous injections require a sufficient fat layer to ensure proper absorption. Muscle mass: Intramuscular injections require a larger muscle mass to ensure proper absorption. Nerve proximity: Avoid injecting near nerves to minimize the risk of nerve damage. Scarring: Rotate injection sites to minimize scarring and promote even absorption. By carefully choosing the injection site and rotating locations, you can enhance the effectiveness of your testosterone injections and reduce potential complications. What is the Best Way to Inject Testosterone? While subcutaneous testosterone injections are by far the most uncomplicated and most comfortable, the more critical question for any TRT patient is how effective this method is and how it affects the potential adverse side effects of TRT. Weekly injections are often recommended to maintain stable hormone levels and reduce side effects. A recent study from the Department of Urology at the University of California (UC) has provided us with such answers. The UC study attempted to answer four questions as they relate to IM vs. SubQ testosterone injections: Comparisons in: Total Testosterone Hematocrit (HCT) Estradiol (E2) Prostate-Specific Antigen (PSA) Two hundred thirty-two men took part in the UC study. Baseline levels were recorded for all men in the four measurement areas and then again at 6-12 weeks post-treatment. The results showed that men who underwent SubQ injections of testosterone resulted in a 14% greater increase in total testosterone levels than the testosterone level of IM patients. SubQ patients also had 41% lower hematocrit post-therapy than IM patients and 26.5% lower E2 levels. For both groups of men, there were no elevated levels of PSA. Additional Studies Comparing IM versus SubQ TRT While the UC study provides valuable data on four specific lab test values of concern and is one of the most recent studies on the topic of subcutaneous versus intramuscular testosterone injections, it is not the only information we have available. An additional Journal of Clinical Endocrinology study found that normal serum testosterone levels were maintained through SubQ injections. Most patients preferred the injection method due to less injection site pain. Similar results were found in a study headed by Dr. Al-Futais in a Canadian study that ran for one year in 2002. Similar results for subcutaneous testosterone injections have also been found in female-to-male (FTM) transgender people-based testosterone studies. The Journal of Clinical Endocrinology and Metabolism reported that FTM patients administering SubQ testosterone were found to easily reach stable and normal testosterone levels along with suitable E2 levels. The study concluded that SubQ testosterone injections are both safe and effective. These findings are particularly relevant for those undergoing gender-affirming hormone therapy, as they highlight the effectiveness and patient preference for SubQ injections. Although far less in-depth than we previously mentioned, a final study of note was published in the Journal of the Endocrine Society. Similar results to the reviews mentioned above were found, along with no significant changes between IM and SubQ patients relating to dihydrotestosterone (DHT). Interestingly, unlike the UC study, this study also measured no notable difference in E2 levels between the two categories. However, it must be noted that this particular study only included a single injection of testosterone undecanoate at 1000 mg. How to Inject Testosterone Using Subcutaneous Injections? If subcutaneous testosterone injections are right for you, you will merely need a small insulin syringe to administer the hormone. A 0.5-inch-long, 25-27 gauge needle in a 1 ml syringe will typically suffice. They also do not require aspiration, commonly used in old IM injection techniques. Unlike IM testosterone injections, SubQ injections do not require aspiration and use a smaller needle. Regardless, the aforementioned insulin needles and syringes are your best choice for comfort and ease of use. Due to the small needle size, you may find it slightly more difficult to draw the testosterone into the insulin syringe. But most men on TRT use 50-100 mg twice per week, which amounts to 0.25 to 0.5 ml of a 200 mg/ml testosterone cypionate or enanthate formulation commonly used in the United States. Those small volumes load up in just 1-2 minutes. Many TRT clinics prescribe protocols to patients to inject their testosterone subcutaneously once or twice weekly. This protocol effectively maintains stable testosterone levels with small, more frequent doses than the old dose of 200 mg once every two weeks. Two injections that split the weekly dose twice per week will suffice for most patients, such as a Monday and Thursday protocol. Is There Any Difference Between Testosterone Cypionate and Testosterone Enanthate? As mentioned early on, testosterone cypionate and testosterone enanthate are the two most commonly prescribed and lowest-cost testosterone esters worldwide. All four studies cited in our discussion were performed using Testosterone Enanthate, excluding the one using Undecanoate. However, using Testosterone Cypionate would have yielded similar, if not identical, results. Both versions of the testosterone hormone are just that, testosterone. Molecularly, there is no difference. It is merely the ester attached, and the carrier oil it may be mixed in is the only difference. Further, as the enanthate and cypionate esters have very similar time-release structures, total serum levels should be relatively the same with either compound, even if injected subcutaneously. Conclusion In conclusion, testosterone replacement therapy is a medical treatment designed to help individuals with low testosterone levels. Administering testosterone injections safely requires proper technique and precautions. Choosing the right injection site is crucial for safe and effective testosterone injections. By understanding the differences between intramuscular and subcutaneous injections, individuals can make informed decisions about their treatment options. Always consult with a healthcare professional before starting testosterone replacement therapy to ensure the best approach for your specific needs. References How to Inject Testosterone Intramuscularly, Shallow IM, or Subcutaneously? Comparison of Outcomes for Hypogonadal Men Treated with Intramuscular Testosterone Cypionate versus Subcutaneous Testosterone Enanthate SIU Academy. Choi E. 10/10/20; 309864; BSP-06.01 Subcutaneous Injection of Testosterone Is an Effective and Preferred Alternative to Intramuscular Injection: Demonstration in Female-to-Male Transgender Patients The Journal of Clinical Endocrinology & Metabolism, Volume 102, Issue 7, 1 July 2017, Pages 2349–2355 Pharmacokinetics and Acceptability of Subcutaneous Injection of Testosterone Undecanoate J Endocr Soc. 2019 Aug 1; 3(8): 1531–1540. -
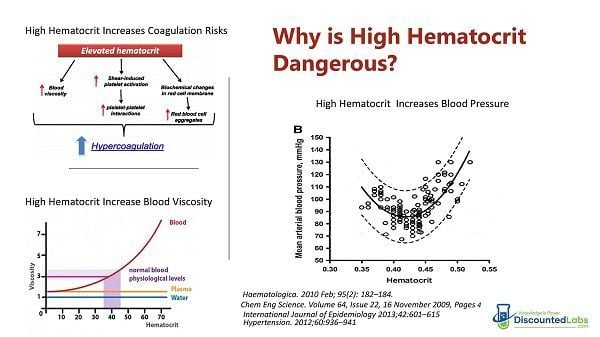
How to Lower High Hematocrit - Effective Strategies
Categories: High Hematocrit , CBC Lab Panel , Testosterone Tests , Testosterone Blood Tests , TRT Blood Tests , Testosterone Lab Tests , Testosterone Replacement Monitoring TestsHigh hematocrit levels, which measure the percentage of red blood cells in the blood, can be signs of several underlying health conditions and they are also a common side effect of testosterone replacement therapy (TRT). High hematocrit levels can increase the risk of developing blood clots, strokes, and other serious complications, especially for those with an underlying condition. Low red blood cell levels, also known as low hematocrit levels, can indicate conditions such as anemia, while high red blood cell levels often signal dehydration and could indicate other conditions, such as polycythemia, increasing a person’s chance of developing blood clots or experiencing blood loss. We will review the different ways to lower the hematocrit and the number of red blood cells on TRT. How to Lower the High Hematocrit Caused by Testosterone Replacement Therapy (TRT) Testosterone replacement therapy (TRT) is one of the most effective ways to combat low testosterone levels, but it's vital that you understand the risks associated with the treatment. As with any form of hormone replacement therapy, there are a few downsides to receiving regular injections of testosterone. One of the main TRT side effects is increased hematocrit, also known as erythrocytosis, which can be a sign of androgen deficiency. This article will explain why this happens, the potential long-term health consequences, and how to prevent or manage this issue. Since abnormally high hematocrit values can pose serious health problems, this article will analyze the correlation between testosterone therapy and high hematocrit. TRT, sleep apnea, smoking, and red blood cell production are contributing factors that can cause high hematocrit that can increase cardiovascular risks if not properly managed. This article explains the basics of how to manage high hematocrit while using testosterone therapy. What is hematocrit? There are several standard ways to measure red blood cells: hematocrit, hemoglobin, and RBC (red blood cell count). All of these are related, and doctors will usually look at two or more. Hematocrit, also referred to as the proportion of red blood cells, is a measurement of how much of a person's blood is made up of red blood cells, also known as whole blood. Hemoglobin, on the other hand, is a density or concentration measurement and is expressed in grams per liter or deciliter. (Hemoglobin is, if you will recall from your high school biology, the iron-based protein that transports oxygen.) RBC is a simple count and is usually expressed as the number of million red blood cells that you have per microliter. Usually, hematocrit is three times the amount of hemoglobin and can be measured through a simple blood sample test. What are the normal ranges for hematocrit? Normal levels of hematocrit for men range from 41% to 50%. normal level for women is 36% to 48%. Why does TRT increase hematocrit? Erythrocytosis is a medical condition that appears when the body makes too many red blood cells. RBCs are responsible for transporting oxygen to organs and tissues. When there are too many, the blood can become too thick and cause cardiovascular complications. There are two types of erythrocytosis: primary and secondary. Problems with the bone marrow, such as bone marrow disease, are typically the cause of primary erythrocytosis. RBCs are made in the bone marrow, and something might trigger an increase in their production. Certain diseases or medications, such as testosterone replacement therapy, can cause secondary erythrocytosis. Some studies concluded that testosterone reduces hepcidin (a hepatic hormone), which is related to iron absorption pathways. When hepcidin is reduced, erythrocytosis is increased [1] An increase in hemoglobin (Hb) and hematocrit (Hct) is indicative of this medical condition. When the Hb is higher than 18.5 g/dL and the Hct is higher than 52% in men, the patient suffers from erythrocytosis. What are the risks of high hematocrit? One of the primary risks of testosterone that you need to be aware of is called polycythemia or erythrocytosis. This is a condition where your body produces too many red blood cells, also known as high hematocrit levels or secondary polycythemia. Hematocrit refers to the percent of red blood cell content in your blood, also known as Hct levels. If your hemocrit levels rise, your blood will become too thick or viscous. This can, in turn, make it more likely that you will develop strokes, heart attacks, and clotting events. Polycythemia is serious and potentially life-threatening if untreated. Since the RBC count is too high in people with erythrocytosis, the blood viscosity also increases, which can lead to various potentially life-threatening medical issues such as venous thromboembolism. This essentially means that tiny blood clots separate from their original source and travel through veins and capillaries, causing blockages that result in stroke, myocardial infarction, or other complications related to reduced blood flow and blood volume. Individuals with high hematocrit levels may also be at risk for conditions such as polycythemia vera, a bone marrow disease that causes an abnormal increase in red blood cells and can lead to symptoms of polycythemia vera such as headache, dizziness, and fatigue. Other potential risks include congenital heart disease, exposure to high altitudes, and reactions to blood transfusions. It can be quite stressful for a man who has finally gotten on TRT, feels better, and then finds out that his hemoglobin is high. Of course, he can always lower his testosterone dosage to try to solve the problem, but this may not be a solution that either doctor or patient wants to pursue. Many men have found that their erectile dysfunction is greatly helped and/or morning erections and libido have returned. The last thing they want to do is lower their dose. So why even worry about a high hemoglobin or RBC count? What’s a few extra red blood cells anyway? Unfortunately, high hemoglobin (or RBCs) is a risk factor for ischemic stroke, i.e., the standard kind of stroke where there is a loss of blood supply to tissues such that permanent damage is usually incurred. [2] Of course, a stroke can be a life-changing (or life-ending) event and should be avoided at all costs. There is also a longer-term risk: elevated hemoglobin could lead to unhealthy iron store levels, which are associated with heart disease and dementia. Iron in tissues can lead to oxidative damage. Just look at what some recent studies have concluded: “Low and high hemoglobin concentrations in older persons are associated with a lower level of cognitive function in old age, particularly in semantic memory and perceptual speed.” [3] “In older persons without dementia, both lower and higher hemoglobin levels are associated with an increased hazard for developing AD [Alzheimer’s Disease] and more rapid cognitive decline.” [4] Can hematocrit stabilize in men on TRT? Hematocrit may stabilize after long-term testosterone replacement. Although there is only one study done in mice, it may explain why hematocrit may eventually decrease and stabilize in men on TRT. There seems to be an adaptive mechanism that makes red blood cell indices change while hematocrit stabilizes. In some men, red blood cell indices (MCV and MCHC) start changing after starting TRT as a way for the body to compensate for the extra production of red blood cells. There are three red blood cell indices: mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC). They are measured by a machine, and their values come from other measurements on a CBC panel. The MCV shows the size of the red blood cells. The MCH value is the amount of hemoglobin in an average red blood cell. The MCHC measures the concentration of hemoglobin in an average red blood cell. [5] Another study that followed frequent blood donors found a reduction in ferritin in them, created as a way for the body to increase iron absorption in the presence of lower hematocrit. Ferritin and hematocrit stabilized after five donations.[6] How to Lower High Hematocrit on TRT Some physicians and TRT guidelines believe that the best way to lower hematocrit is to stop TRT. But stopping TRT can have negative consequences in the quality of life, as men who do so tend to stay hypogonadal for months, and most do not return to “normal levels.”. Fortunately, there are several ways to decrease high hematocrit and also potentially prevent it from happening. Give Blood. This is a time-proven technique for men on testosterone therapy to lower their hemoglobin levels. And you are helping out someone else while you’re doing it! Every unit of blood donated can decrease hematocrit by 3 points, which is equivalent to one pint of blood. However, be careful not to donate more frequently than every 2.5 months, as the Red Cross advises, to prevent losing too much iron and ferritin, which can cause fatigue in men using testosterone therapy. You can check your iron and ferritin levels with this iron blood test. It's recommended that you donate when you are in the 51–52 hematocrit range. However, some organizations (like the Red Cross) will reject blood with a hematocrit higher than 53%, so it is good to avoid that high hematocrit level if you want to donate blood. Men who are rejected from blood donations because of high hematocrit can still give blood if their physicians call in an order for a therapeutic phlebotomy at the local blood center. Lower Your TRT Dose. If you have high hemoglobin or hematocrit from testosterone therapy, then your doctor may require you to lower your dose. This is not always a bad thing, as some men are actually taking more testosterone than they actually need, which can lead to side effects in both the long and short term. Drink Water. It is important to remember that hemoglobin is very dependent on your hydration levels. If you were dehydrated when you had your blood drawn, this could have made things worse. If you think you were dehydrated, discuss a retest with your doctor. Treat Thyroid Issues. Hypothyroidism (low thyroid function) can lower your RBC counts, and hyperthyroidism (high thyroid function) can raise them, too. If you haven’t checked your thyroid function lately, this might be wise. And don’t forget to get a full thyroid panel, including thyroid antibodies, if you can afford it. [10] Consider transdermal (topical) or oral testosterone. One research summary stated that topical testosterone creams or gels increase hematocrit, in general, less than intramuscular testosterone injections: “Intramuscular testosterone is the only form that significantly increases hematocrit above normal levels. However, it does so strongly, with up to a 6% change from baseline. The runner-up is testosterone gel, with an average increase of 2.5% over baseline levels.” [7]. Therefore, if you are on intramuscular injections and struggling with high hematocrit or hemoglobin, going on topicals may help a little. Discuss with your physician. NOTE: A cheap alternative is Compounded Testosterone Creams and Gels. Another emerging option is oral testosterone products. Switch from intramuscular injections to lower-dose subcutaneous Subcutaneous Testosterone Injections. Two hundred thirty-two men took part in a University of California study. Baseline levels were recorded for all men in each of the four measurement areas and then again at 6–12 weeks post-treatment. The results showed that men who underwent subcutaneous testosterone (SubQ) injections had a 14% greater increase in total testosterone levels compared to the testosterone levels of intramuscular testosterone injection (IM) patients. SubQ patients also had a 41% lower hematocrit post-therapy than IM patients and 26.5% lower estradiol levels. For both groups of men, there were no elevated levels of PSA. [7] Avoid or Reduce the Consumption of Red Meats. It is interesting because one of the criticisms that meat eaters level against vegetarians is that plant foods have many “anti-nutrients” that can slow down or bind with minerals such as iron. For example, organizations like Weston Price love to castigate vegetarians for their phytic acid consumption. Phytic acid is present in plant foods and binds to iron, magnesium, phosphorous, and calcium. It can, if overconsumed, lead to mineral deficiencies. However, Dr. Bernard points out that usually, it is likely very health-protective for most people because these minerals, as in the case of zinc and iron, are neurotoxic at even relatively low levels of tissue accumulation. Research has also shown that too much iron also contributes to heart disease, and there may be a link to colon cancer as well. [8]So, avoiding red meats, which are high in iron, stands a good chance of lowering your hemoglobin scores and protecting your long-term health unless some other preventative action is taken (such as giving blood). Actual dietary studies are required to support this statement. As a verification, one study of vegetarians and non-vegetarians found that females had significantly lower hemoglobin levels. Males had lower levels, but it may not have been statistically significant. [8] However, another study was more definitive and concluded: “It was found that hemoglobin, hematocrit, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, white blood cells, neutrophils, serum ferritin, and serum vitamin B12 in vegetarians were significantly lower than control subjects.” [11] Ferritin is a key measure, by the way, because it indicates that tissue levels of iron are lower and thus will likely cause less permanent damage. (This study did show that some vegetarians were iron deficient, as should be noted.) Fix Sleep Apnea. Sleep apnea can cause depleted oxygen saturation values that can enhance the body's ability to produce more red blood cells and hemoglobin as a way to compensate for the low blood levels of oxygen during the sleep cycle. And, sure enough, there are studies that confirm this as well. [12] So, if your hematocrit, hemoglobin, or RBCs are running high, think about getting tested for sleep apnea. A recent study commented that “one possible explanation is that repeated episodes of nocturnal hypoxia (low oxygen condition) lead to a hypercoagulable state that predisposes patients to thrombotic (blood clotting) events. There is evidence supporting a wide array of hematological changes that affect hemostasis (e.g., increased hematocrit, blood viscosity, platelet activation, clotting factors, and decreased fibrinolytic activity).” Reduce Inflammation. Hepcidin, the iron absorption-modulating hormone, can be decreased even further by inflammation. Checking for infections, CRP levels, etc., and then treating the underlying cause may help. [13] Consider Curcumin (Turmeric). Turmeric or curcumin, is increasingly studied as an anti-inflammatory and anti-cancer agent. It binds to ferric iron in the gut and causes iron deficiency in mice. A case history reported a possible case of iron deficiency anemia in a human taking turmeric. [14] Stop Smoking. Smoking reduces the amount of oxygen in the blood and makes the body produce more red blood cells and hemoglobin to compensate for that lower oxygen saturation.[14] Treat High Blood Pressure with Losartan. If you have high blood pressure, consider taking Losartan.[15] Losartan can be safely and effectively used to normalize hematocrit in patients with COPD and erythrocytosis, an effect that could obviate the need for therapeutic phlebotomy. Consider Grapefruit. Grapefruit extract (narigin) may decrease hematocrit [16]. There was no significant difference between ingesting 1/2 or 1 grapefruit per day, but a decrease in hematocrit due to ingestion of grapefruit was statistically significant at the p less than 0.01 level. However, discuss with your physician the fact that grapefruit can increase the blood levels of medications. The most important message of this article is that monitoring hematocrit every few months is a smart way to minimize cardiovascular risks associated with high hematocrit. You can buy your hematocrit and related tests on DiscountedLabs.com at affordable prices. Hematocrit is included in the CBC and other panels on Discounted Labs: Get Your Hematocrit Test Now Testosterone, Hematocrit, Ultrasensitive Estradiol and Prolactin Panel Hematocrit + Total and Free Testosterone References The Journal of Clinical Endocrinology & Metabolism, Volume 95, Issue 10, 1 October 2010, Pages 4743–4747 Eur Neurol, 1996, 36(2):85-8. Neuroepidemiology, 2008 December, 32(1): 40 46, “ Relation of Hemoglobin to Level of Cognitive Function in Older Persons” Neurology, 2011 Jul 19, 77(3):219-26, “Hemoglobin level in older persons and incident Alzheimer disease: prospective cohort analysis. Endocrinology. 2015 May; 156(5): 1623–1629. TRANSFUSION 2008; 48: 2197-2204. Comparison of Outcomes for Hypogonadal Men Treated with Intramuscular Testosterone Cypionate versus Subcutaneous Testosterone Enanthate SIU Academy. Choi E. 10/10/20; 309864; BSP-06.01 International Journal of Natural and Applied Sciences Vol. 2 (3) 2006: pp. 174–177, “Comparative study of the hemoglobin concentration of vegetarian and non-vegetarian subjects in Ogun state, Nigeria” World J Gastroenterol, 2006 September 21, 12(35): 5644-5650, “Hemoglobin induces colon cancer cell proliferation by release of reactive oxygen species” Iran J Ped Hematol Oncol, 2013; 3(2):73-77, “Effect of Thyroid Dysfunctions on Blood Cell Count and Red Blood Cell Indices” J Med Assoc Thai, 1999 Mar, 82(3):304-11, “Hematological parameters, ferritin and vitamin B12 in vegetarians” Can Respir J. 2011 Nov-Dec; 18(6): 338-348, “Coagulability in obstructive sleep apnea” Am J Kidney Dis. 2012;59(3):444-451 -
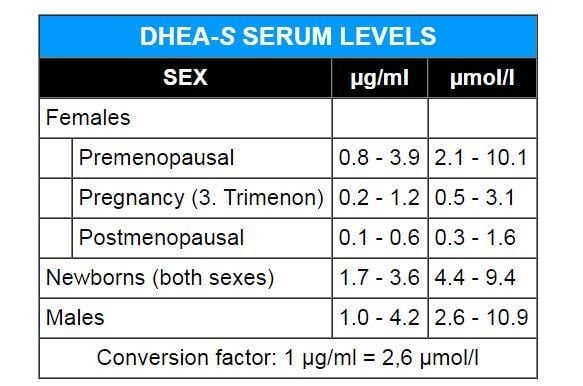
DHEA Supplement: Is It Right for You?
Categories: DHEA Lab Test , Fatigue Blood Tests , lab tests for women , Women's Hormone Tests , Men's Health Lab TestsDHEA Levels: Do You Need to Take a Supplement? The dehydroepiandrosterone sulfate (DHEA-S) test checks how much DHEA-S is in the blood. The adrenal gland produces the hormone DHEA-S. It is a building block for androgens and estrogens. The test is generally done to check how well the adrenal glands are working and to look into conditions that might cause hormone production to be off. DHEA-S test, also known as the test DHEA sulfate, can help figure out what's causing irregular periods, infertility, and a low libido. It is also used to find out if someone has a growth in their adrenal gland, congenital adrenal hyperplasia, or polycystic ovary syndrome. People on long-term glucocorticoid medicine can also use the test to check how well their adrenal glands are working. It is an important test for people who think their hormones might be out of order. What is DHEA? The adrenal glands also produce dehydroepiandrosterone (DHEA), the most abundant hormone found in the blood stream. Your adrenal glands and, to a lesser extent, your ovaries and testes produce the hormone known as DHEA. DHEA is changed into DHEA-S in your adrenal glands and liver. The body uses DHEA as the starting material for producing the sex hormones testosterone and estrogen. However, DHEA supplementation studies have shown that it only increases testosterone in women. The production of DHEA diminishes in most people after age 40. DHEA levels typically decrease with age in both men and women, highlighting its significance in hormone testing and the evaluation of conditions affecting adrenal function and hormonal balance. In people aged 70 years, DHEA levels will be approximately 30 percent lower than what they were at age 25. Low blood levels of DHEA have been associated with many degenerative conditions, making it a popular supplement for those undergoing in-vitro fertilization (IVF) treatments. Understanding DHEA and Its Role in the Body DHEA is a hormone produced by the adrenal glands, which are small glands located on top of each kidney. These glands are responsible for producing most of the body's DHEA, with smaller amounts being produced by the testicles in men and ovaries in women. DHEA plays a crucial role in the production of sex hormones, including testosterone and estrogen, which are essential for the development of male and female sex characteristics. As we age, DHEA levels naturally decline, with the highest levels typically occurring during puberty. This decline can lead to a range of symptoms, including decreased libido, fatigue, and weight gain. However, it's important to note that DHEA supplements are not recommended as a way to prevent aging-related conditions, as there is no reliable evidence to support their effectiveness. While some people may seek out DHEA supplements to counteract these symptoms, it's crucial to approach supplementation with caution and under the guidance of a healthcare professional. DHEA is a hormone produced by the adrenal glands DHEA plays a crucial role in the production of sex hormones DHEA levels naturally decline with age The Importance of DHEA Sulfate (DHEAS) DHEAS is the most abundant form of DHEA in the body, accounting for approximately 90% of the total DHEA present. Produced by the adrenal glands, DHEAS is converted into DHEA in the body. The DHEA sulfate test measures the levels of DHEAS in the blood, which can help diagnose adrenal disorders and evaluate adrenal function. DHEAS plays a crucial role in regulating the reproductive system. Abnormal levels can lead to a range of symptoms, including excess hair growth, male pattern baldness, and deepening of the voice in women. In men, high levels of DHEAS can cause early puberty, while low levels can lead to erectile dysfunction and decreased libido. In women, high levels of DHEAS can cause polycystic ovary syndrome (PCOS), a condition characterized by irregular menstrual periods, excess hair growth, and infertility. Low levels of DHEAS can lead to adrenal insufficiency, a condition where the adrenal glands do not produce enough hormones. The DHEA sulfate test is typically ordered by a healthcare provider if symptoms indicate an adrenal disorder or adrenal tumor. The test involves a blood sample, which may cause moderate pain, a prick or sting, and possibly some throbbing or bruising after the needle is inserted. The test is usually performed at a doctor's office or another medical setting, and the results are typically available within a few business days. Normal blood levels of DHEAS can differ by sex and age, with typical normal ranges for females being 20-150 mcg/dL and for males being 30-450 mcg/dL. Abnormal levels of DHEAS can indicate a range of conditions, including adrenal gland disorders, pituitary gland disorders, and congenital adrenal hyperplasia. In conclusion, DHEA and DHEAS play crucial roles in the body, and abnormal levels can lead to a range of symptoms and conditions. The DHEA sulfate test is an essential tool for diagnosing adrenal disorders and evaluating adrenal function. If you're experiencing symptoms related to adrenal disorders, it's essential to consult with a healthcare provider to determine the best course of action. DHEAS is the most abundant form of DHEA in the body Who Can Benefit from Taking DHEA Supplements? Some controversial and non-conclusive studies have shown that people with immune deficiencies and fatigue may benefit from supplementation with this hormone. It is also believed to help correct some adrenal problems, such as changes in blood pressure, caused by conditions such as adrenal insufficiency. It is still available over-the-counter in the United States. Due to a recent congressional bill classifying it as a performance-enhancing steroid (despite the fact that no studies have demonstrated that it has such an effect), this might soon change. One study showed that women with the correct levels of DHEA can convert it into testosterone as their body needs it, while men do not benefit to the same degree. You need a blood test to know if you have low DHEA-S since most of the DHEA converts into this sulfated form. Common doses for women are 5 to 30 mg a day, while men tend to benefit from 25–100 mg per day (to bring low levels of DHEA-S to normal) DHEAS was the only hormone significantly negatively correlated to the prevalence of erectile dysfunction among 17 investigated hormones, including testosterone and estradiol, in the large and long-term Massachusetts Male Aging Study. In addition, a study done by Dr. Basar et al., which included 348 male patients, reported that DHEAS and free testosterone levels were significantly lower in men with sexual dysfunction. However, evidence of the positive effects of DHEA supplementation on improving sexual function in men is unconvincing, scanty, and conflicting. Only 4 placebo-controlled studies have been performed to investigate the effect of supplementing DHEA on improving libido in men. Unfortunately, the data from these studies did not show any difference in sexual desire in men. The limited effect of DHEA on male sexual function is not surprising. In fact, the specific DHEA contribution to the overall circulating testosterone level in men is marginal, if not negligible. A double-blind, placebo-controlled study was done on male and female patients with low thyroid function (hypopituitary) who were given growth hormone (GH) along with 50 mg of DHEA. When DHEA was replaced in female patients, the dose of GH dropped by 14.6 +/- 20% while serum IGF-I stayed the same (P < 0.05). This was maintained for 12 months, and there was a significant fall in serum IGF-I two months after the withdrawal of DHEA. There was no change in the male group. Do not use DHEA supplements unless your blood levels of DHEA-S are low. If low, start at a low dose and get your DHEA-S tested again after a month. Men who use DHEA supplements may have problems with higher estrogen levels since this hormone can also be metabolized into estradiol. This could result in gynecomastia and water retention. If you start taking DHEA, have your blood levels checked to make sure they are not above normal. Additionally, individuals with a history of hormone-sensitive cancers, such as breast or prostate cancer, should consult with their doctor before taking a DHEA supplement. There are many claims about DHEA being an anti-aging and anti-cancer cure, but none of these claims have been substantiated with strong data. How Do You Know Your DHEA Blood Level with a DHEA Sulfate Test? The standard blood test to evaluate DHEA status is one that measures DHEA sulfate levels (dehydroepiandrosterone sulfate, or DHEA-S). DHEA-S is calculated in micrograms per deciliter (µg/dL) of blood. A DHEA-S blood test may be taken three to six weeks after initiating DHEA to help determine optimal dosing. DHEA testing may save you money if it shows you can take less DHEA to maintain youthful DHEA serum levels. Some tests may exhibit interference when sample is collected from a person who is consuming a supplement with a high dose of biotin (also termed as vitamin B7 or B8, vitamin H or coenzyme R). Patient should be cautioned to stop biotin consumption at least 72 hours prior to the collection of a sample. Potential Benefits of DHEA Supplementation Low DHEA and Adrenal Insufficiency Adrenal insufficiency is a condition in which the adrenal glands do not produce enough of the hormone DHEA. In such cases, doctors may prescribe DHEA supplements to help alleviate symptoms and improve quality of life. The National Collegiate Athletic Association has banned the supplement, but studies have shown that it may be useful in treating lupus and adrenal insufficiency (Philadelphia, PA: Elsevier). However, further research is still needed to determine its effectiveness in treating these conditions. DHEA and Depression DHEA (dehydroepiandrosterone) supplements have been studied for their potential to alleviate depressive symptoms. The test DHEA sulfate can help diagnose adrenal disorders that may contribute to depressive symptoms. Studies have found that DHEA-S levels are associated with depressive symptoms in women in the late reproductive years. A systematic review and meta-analysis of randomized controlled trials showed that DHEA may be effective in treating depressive symptoms in various psychiatric and medical illnesses. However, further research is needed to fully understand the effects of DHEA on depression and its potential as a treatment option, making DHEA treatment a potential option for those struggling with depressive symptoms. DHEA in Elderly Men A DHEA supplement has been found to be beneficial for elderly men. Studies have shown that elevated serum dehydroepiandrosterone sulphate levels correlate with an increased risk for metabolic syndrome in elderly men. DHEA supplements can also produce small decreases in fat mass in elderly men, although more research is needed to confirm this finding. Additionally, taking DHEA supplements may also have an effect on body weight and fat burning, but the evidence is unclear. It is important to consult a healthcare professional before taking any DHEA supplements, especially for elderly men with pre-existing medical conditions or those taking other medications. DHEA supplements have been suggested to slow down the aging process by maintaining DHEA levels in the body. Although some small studies have reported positive anti-aging effects from the use of DHEA supplements, others have not shown any effect. According to the Natural Medicines Comprehensive Database, there is no conclusive evidence that DHEA supplements affect the aging process. DHEA is a precursor for the production of estrogens and androgens, and its production decreases with the aging process, which makes it a controversial topic among researchers regarding its use in postmenopausal women. DHEA and Bone Density A DHEA supplement has been studied for its potential to improve bone mineral density in older women. Studies have produced mixed results, but some suggest that DHEA may increase bone mineral density in the hip and thigh bones of females. This effect seems to increase with higher doses of the supplement. DHEA can be expressed via sex steroid receptors and androgen and estrogen receptors and plays a role in bone cell proliferation and differentiation. The activation of androgen receptors can stimulate bone cell growth, which may contribute to improvements in mineral density. DHEA and Bodybuilding DHEA often gets marketed as a "muscle builder" to men. As a muscle-building supplement in young, healthy men, DHEA is essentially worthless, and high intakes may in fact be counterproductive to gaining muscle as high doses also cause an increase in estrogen and the effects on testosterone are minimal. Studies have been conflicting in this area at best, and most "real world" users report no improvements in strength, muscle mass, etc. from using DHEA, with little evidence to support its effectiveness. As a supplement that can improve mood, libido, memory, and possibly alter body composition (i.e., increase muscle, improve bone density, and reduce body fat), DHEA appears to be an option to explore for women. Most of the research has been done in DHEA-deficient populations, but data and real-world experience suggest it's also beneficial to women who are not medically deficient in this hormone, particularly in improving sex drive. Although the benefits of this hormone to women come predominately from its conversion to testosterone, it also appears that some of the effects may be due to other mechanisms. DHEA Potential Interactions Yes, it is important to be aware of potential interactions with other medications or supplements when taking a DHEA supplement. DHEA can interact with several types of medications like blood thinners, insulin, and corticosteroids. It may also affect the effectiveness of certain herbal supplements, like ginkgo biloba and saw palmetto. People with liver problems should also avoid taking DHEA, as it is metabolized in the liver. It is advisable to consult with a healthcare professional before starting any new supplement regimen to ensure there are no adverse effects or interactions with existing medications or supplements. How Long Does It Take for DHEA to Work? The length of time it takes to see results from taking a DHEA supplement can vary depending on multiple factors. Some people may notice an improvement in their symptoms within just a few days, while others may need to take the supplement for several weeks or even months before seeing any noticeable changes. It is important to speak with a healthcare professional before starting any new supplement regimen to determine the appropriate dosage and monitor any potential side effects. Additionally, it's important to keep in mind that DHEA supplements are not appropriate for everyone and that those who are pregnant, nursing, or have certain medical conditions should avoid taking them. DHEA Dosage The recommended dosage for a DHEA supplement varies depending on age, gender, and health conditions. Generally, the recommended dosage for men is 50–100 mg per day, while women are advised to take 25–50 mg per day. However, it is important to consult with a healthcare provider before starting any supplement regimen. Additionally, it is recommended to take DHEA supplements in the morning as the body naturally produces more DHEA during this time. It is also suggested to cycle DHEA use, taking it for three weeks and then pausing for one week before resuming. different individuals. Its role in supporting adrenal function, potentially aiding in conditions like adrenal insufficiency and depression, and influencing bone density and sexual health, offers hope for specific groups, especially postmenopausal women and the elderly. However, it's crucial to approach DHEA supplementation with caution and informed understanding. Men, particularly, may find limited benefits and should be wary of potential side effects like increased estrogen levels. Conclusion Before considering DHEA supplements, it's essential to get your DHEA-S levels tested. This is where DiscountedLabs.com can be an invaluable resource, offering affordable and convenient blood tests without the need for a doctor's visit in several U.S. states. Understanding your DHEA-S levels is the first step in determining whether supplementation is right for you. Remember, while DHEA has potential benefits, it's not a one-size-fits-all solution. Consult with healthcare professionals, consider potential interactions with other medications or supplements, and monitor your body's response to supplementation. As we continue to explore the benefits and limitations of DHEA supplements, it's essential to make informed, health-focused decisions, aided by reliable testing and professional advice. Turn to DiscountedLabs.com for your testing requirements if you're thinking about taking DHEA supplements so that you can make informed health decisions.